Download
1 / 50
500 likes | 743 Views
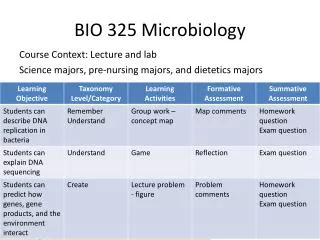
Microbiology Revision – Lecture 1. Dr Anna Goyder and Dr Helen McKenna 19/03/13 - 21/03/13. Outline. 2 lectures x 90mins each: Bacteria and Abx Viruses and Antivirals Vaccinations Infections by system: - CNS - Cardio - Resp - GI/hepatitis - GU/gynae - Musculoskeletal

E N D
Microbiology Revision – Lecture 1 Dr Anna Goyder and Dr Helen McKenna 19/03/13 - 21/03/13
Outline 2 lectures x 90mins each: Bacteria and Abx Viruses and Antivirals Vaccinations Infections by system: - CNS - Cardio - Resp - GI/hepatitis - GU/gynae - Musculoskeletal Mycobacterial Zoonoses Malaria
Bacteria simplified Gram positive Cocci staphylococcus streptococcus enterococcus Rods/bacilli ABCDL (see next slide) Gram negative Cocci the diplococci - neisseria (gonorrhoea, meningitidis ‘meningococcus’), moraxella Rods/bacilli ENTERICS - E Coli, salmonella, shigella, klebsiella, proteus, campylobacter, helicobacter, vibrio… ie most other things! Coccobacillihaemophilus, legionella, brucellosis, bordetella, chlamydia* rickettsia* *obligate intracellular Spiral spirochetes – treponema (syphilis), leptospira (Weil’s), borrelia (lyme)
Gram + rods:ABCDL Actinomyces Bacillus (anthracis, cereus) Clostridium (difficile, botulinum, perfringens) Diphtheria (corynebacterium diphtheriae) Listeria
Diplococcus Moraxella Neisseria
Anaerobes WHAT ARE THEY?
Anaerobes Do NOT require O2 for growth Therefore suspect them in unhealthy/dying tissues/reduced blood supply, necrotic tissue From GI tract including mouth E.g. suspect in bites, Foul smell! Free gas under skin! Nasty Treat with metronidazole, cephamycins (cefoxitin, cefotetan, cefmetazole, flomoxef) Aminoglycosides do NOT cover anaerobes – O2 needed for them to enter the cell.
Anaerobes OBLIGATE CANNOT use O2/grow where there is oxygen Bacteroides Clostridium Actinomyces • FACULATIVE • Can grow where there is OR isn’t oxygen • Staphylococcus, E. Coli, Listeria
Antimicrobials Antibiotics Antivirals Antifungals
Antibiotics (antibacterials) A) Cell wall synthesis inhibitors B) Protein synthesis inhibitors C) DNA synthesis inhibitors D) RNA synthesis inhibitors E) Anti-folate drugs
Antibiotics (antibacterials) A) Cell wall synthesis inhibitors B) Protein synthesis inhibitors C) DNA synthesis inhibitors D) RNA synthesis inhibitors E) Anti-folate drugs
A. Cell wall synthesis inhibitors β-lactams 1. Penicillins 2. Cephalosporins Crossreactivity – caution if hx anaphylaxis 1st generation – gram + > - 2nd generation – gram + and - 3rd generation – gram - > + - have T in them – T for ‘third’ cefotaxime, ceftazidime, ceftriaxone 3. Carbapenems B R O A D spectrum Glycopeptides Require therapeutic drug monitoring (TDM) 1. Vancomycin Usually IV – covers MOST GRAM + incl MRSA - but NOT VRE! Exception - oral vancomycin – for C. Difficile diarrhoea (where metronidazole has failed) 2. Teicoplanin
Antibiotics (antibacterials) A) Cell wall synthesis inhibitors B) Protein synthesis inhibitors C) DNA synthesis inhibitors D) RNA synthesis inhibitors E) Anti-folate drugs
B. Inhibitors of protein synthesis 5 to remember: 1. Macrolides 2. Tetracyclines 3. Aminoglycosides 4. Chloramphenicol 5. Oxazolidinones erythromycin, clarithromycin, azithromycin doxycycline, lymecycline gentamicin, amikacin – TDM needed (for your EYES only) Linezolid – don’t need to know any more
Antibiotics (antibacterials) A) Cell wall synthesis inhibitors B) Protein synthesis inhibitors C) DNA synthesis inhibitors D) RNA synthesis inhibitors E) Anti-folate drugs
C. DNA synthesis 1. Quinolones – Ciprofloxacin, Moxifloxacin, Levofloxacin(thinkCiprofloxaquin, Moxifloxaquin etc) Act on DNAGyrase Active mostly against Gram negatives – use for UTIs, bacterial gastroenteritis 2. Nitroimidazoles – Metronidazole Useful against anaerobes and protozoa 3. Nitrofurantoin - UTIs
Antibiotics (antibacterials) A) Cell wall synthesis inhibitors B) Protein synthesis inhibitors C) DNA synthesis inhibitors D) RNA synthesis inhibitors E) Anti-folate drugs
D. RNA synthesis Rifampicin, Rifabutin Treatment - as part of combination therapy because resistance develops quickly – mycobacteria – TB Prophylaxis – single agent - Meningococcal
Antibiotics (antibacterials) A) Cell wall synthesis inhibitors B) Protein synthesis inhibitors C) DNA synthesis inhibitors D) RNA synthesis inhibitors E) Anti-folate drugs
E. Anti-folate drugs Trimethoprim UTIs Sulphonamides Co-trimoxazole ‘Septrin’ = Trimethoprim + Sulphamethoxazole P. Jiroveci prophylaxis in AIDs
TB treatment RIPE – Rifampicin, Isoniazid, Pyrazinamide, Ethambutol Normally 2m of 4 drugs, then 4m of 2 drugs Exceptions –spinal (12 months), MDR TB (minimum 18 months) Side Effects – - Ethambutol - E for Eye – optic neuritis R/I/P – hepatotoxicity Isoniazid – peripheral neuropathy – co-prescribe pyridoxine
Classification DNA viruses Double-stranded: Adenovirus Herpes virus Pox viruses Double-stranded plus reverse transcriptase: Hepadnavirus Single stranded: Parvovirus RNA viruses Double-stranded: Reovirus (+)Single-stranded: Picornavirus Togavirus Flavivirus (+) Single-stranded plus reverse transcriptase: Retrovirus (-)Single-stranded: Orthomyxovirus Paramyxovirus Rhabdovirus
Classification DNA viruses Double-stranded: Adenovirus Herpes virus (LATENT) Pox viruses Double-stranded plus reverse transcriptase: Hepadnavirus Hepatitis B Single stranded: Parvovirus B19 – slapped cheek, 5th disease RNA viruses Double-stranded: ReovirusRotavirus (+) Single-stranded PicornavirusEnteroviruses(polio, echo, coxsackie), rhinovirus, Hepatitis A TogavirusRubella Flavivirus Hepatitis C, Dengue, Yellow Fever (+) Single-stranded plus reverse transcriptase: Retrovirus HIV 1, 2; HTLV1 (-)Single-stranded: OrthomyxovirusInfluenza A, B, C ParamyxovirusMeasles, Mumps, RSV RhabdovirusRabies
Questions Which herpes virus? A HHV 1/HSV 1 B HHV 2/HSV 2 C HHV 3/ VZV D HHV 4/ EBV E HHV 5/CMV F HHV 6/ Roseola G HHV 7 H HHV 8 • A 50 year old man presents to HIV clinic with a widespread purple rash • A 6 year old child presents with 1 week of fever and malaise and develops crops of vesicles on scalp and mouth • 18 year old student presents with excessive fatigue and repeated bouts of pharyngitis. He is found to have cervical lymphadenopathy and enlarged spleen. • 1 week old baby, not feeding, vesicular lesions on face and mouth. Mother had painful genital rash in last week.
Antivirals HSV: Encephalitis, Disseminated (Genital, Oal) VZV: immunocompromise, pregnancy, pneumonitis Aciclovir Guanosine analogue- Blocks viral DNA extension Requires activation by viral TK CMV (lacks TK) Ganciclovir Resistant: Foscarnet
Antivirals HAART Triple therapy – usually 2xNRTI + NNRTI/PI Start when CD4 count <250 NRTIs end in –ine (exceptions: tenofovir and abacavir) NNRTIs – nevirapine, efavirenz PIs end in -vir (exceptions: tenofovir and abacavir = NRTIs)
UK Schedule DTaP/IPV/Hib 2, 3, 4 months PCV 2, 4 months Men C 3, 4 months Hib + MenC 12 months booster MMR + PCV 12-13 months DTaP/IPV/MMR 3-5 years BCG high risk babies, 10-14y HPV (16 and 18 - oncogenic) girls 12-13y DT + IPV 13-18 years Rubella seronegative women
Which of the following is a LIVE vaccine? A Diphtheria B Yellow fever C Rabies D Tetanus E Pertussis
Breaktime • 5 mins • Only go to the toilet if you’re desperate • Don’t talk about medicine • Talk about something else • Might be a good time to start filling in your feedback form
SYSTEMS CNS (including prion disease) Heart Respiratory Tract Gastrointestinal Tract Urinary Tract Sexually transmitted diseases Musculoskeletal and skin
Meningitis • Treat empirically as soon as possible: • CEFTRIAXONE • + VANCOMYCIN if possible penicillin-resistance pneumococci • + AMPICILLIN if immunocompromised (suspect Listeria) • (Neonate: cefotaxime and amoxicillin) • CONTACTS: rifampicin. • 2. Lumbar Puncture • Contraindicated if clinical evidence of raised ICP • CT • 3. Vaccine: Hib, MenC
Questions 50 year old man Headache and neck stiffness CT brain normal LP – opening pressure 15 cmH20 CSF: Cloudy WCC 100 (70% lymphocytes) Protein 0.7 Glucose 3.3 (serum glucose 4.7) Diagnosis? A Bacterial meningitis B Viral meningitis C TB D Normal CSF E Cryptococcal
20 year old man Headache and sore throat Fever Photophobia CSF: Clear Lymphocytes 2; Polymorphs 0 Protein 0.3 Glucose 4.1 (serum glucose 5.9) Diagnosis? A Guillian-Barre Syndrome B Viral meningitis C Bacterial meningitis D Cerebral Malaria E Normal CSF
Which of the following types of viral meningitis may be associated with a characteristically LOW CSF glucose level? A Mumps B CMV C Measles D HIV E Echovirus
Prion disease: Infectious protein Causes rapid neurodegeneration (Dementia, ataxia) No inflammatory/immune reaction
Questions Which of the following statements about variant CJD is true? A Mainly affects the elderly B More rapidly progressive than sporadic CJD C Initial symptoms are always neurological D Tonsillar biopsy is often diagnostic E EEG is usually abnormal
Which of the following statements is true? A Familial CJD is more rapidly progressive than sporadic CJD B Familial CJD is inherited in a recessive fashion C Familial prion disease does not cause ataxia D All cases of variant CJD are methionine homozygous at codon 129 E Tonsillar biopsy is used to diagnose sporadic CJD
Endocarditis Subacute versus acute General points – Blind therapy – fluclox/benpen/vancomycin + gent If penicillin allergic/MRSA - use vancomycin Mortality – 30% with staph, 5% with strep
Culture-negative Endocarditis • Caused by A) taking blood cultures AFTER starting antibiotics B) Organisms difficult to culture: brucella, coxiella, chlamydia, mycoplasma, HACEK organisms: Haemophilus, Actinobacillus, Cardiobacterium, Eikenella Kingella -> do serology
That’s all for now • Please fill in a feedback form if you have not done so already