Download
1 / 1
10 likes | 182 Views
CERVICAL ECTOPIC: CASE REPORT Ling Yien Hii, Carol Lim, Soon Ruey SABAH WOMEN’S AND CHILDREN’S HOSPITAL, KOTA KINABALU, SABAH. PRESENTED AT 10 TH RCOG INTERNATIONAL SCIENTIFIC MEETING 6 – 8 JUNE 2012, BORNEO CONVENTION CENTRE KUCHING, KUCHING, SARAWAK, MALAYSIA.

E N D
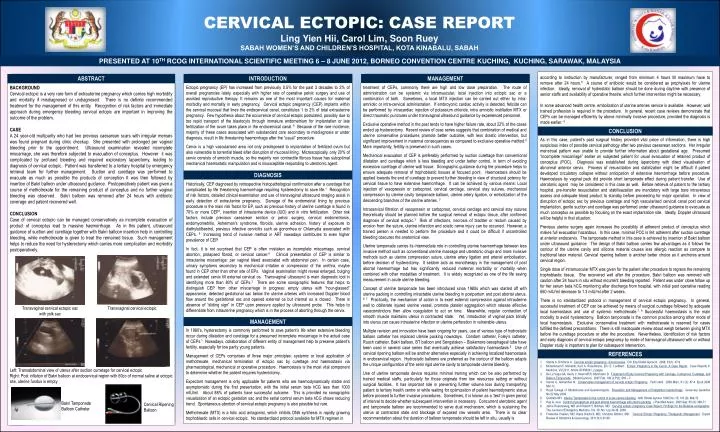
CERVICAL ECTOPIC: CASE REPORT Ling Yien Hii, Carol Lim, Soon RueySABAH WOMEN’S AND CHILDREN’S HOSPITAL, KOTA KINABALU, SABAH PRESENTED AT 10TH RCOG INTERNATIONAL SCIENTIFIC MEETING 6 – 8 JUNE 2012, BORNEO CONVENTION CENTRE KUCHING, KUCHING, SARAWAK, MALAYSIA according to instruction by manufacturer, ranged from minimum 4 hours till maximum have to remove after 24 hours.5 A course of antibiotic would be considered as prophylaxis for uterine infection. Ideally, removal of hydrostatic balloon should be done during daytime with presence of senior staffs and availability of operative theatre, which further intervention might be necessary. In some advanced health centre, embolization of uterine arteries service is available. However, well trained profession is required in the procedure. In general, recent case reviews demonstrate that CEPs can be managed efficiently by above minimally invasive procedure, provided the diagnosis is made earlier. 4 ABSTRACT INTRODUCTION MANAGEMENT BACKGROUND Cervical ectopic is a very rare form of extrauterine pregnancy which carries high morbidity and mortality if misdiagnosed or undiagnosed. There is no definite recommended treatment for the management of this entity. Recognition of risk factors and immediate approach during emergency bleeding cervical ectopic are important in improving the outcome of the problem. CASE A 24 year-old multiparity who had two previous caesarean scars with irregular menses was found pregnant during clinic checkup. She presented with prolonged per vaginal bleeding prior to the appointment. Ultrasound examination revealed incomplete miscarriage, she was therefore subjected to evacuation of conceptus. However it was complicated by profused bleeding and required exploratory laparotomy, leading to diagnosis of cervical ectopic. Patient was transferred to a tertiary hospital by emergency retrieval team for further management. Suction and curettage was performed to evacuate as much as possible the products of conception It was then followed by insertion of Bakri balloon under ultrasound guidance. Postoperatively patient was given a course of methotrexate for the remaining product of conceptus and no further vaginal bleeding was observed. Bakri balloon was removed after 24 hours with antibiotic coverage and patient recovered well. CONCLUSION Case of cervical ectopic can be managed conservatively as incomplete evacuation of product of conceptus lead to massive haemorrhage. As in this patient, ultrasound guidance of suction and curettage together with Bakri balloon insertion help in controlling bleeding, while methotrexate is given to treat the remained tissue. Such management helps to reduce the need for hysterectomy which carries more complication and morbidity postoperatively. Ectopic pregnancy (EP) has increased from previously 0.5% for the past 3 decades to 2% of overall pregnancies lately, especially with higher rate of operative pelvic surgery and use of assisted reproductive therapy. It remains as one of the most important causes for maternal morbidity and mortality in early pregnancy. Cervical ectopic pregnancy (CEP) implants within the cervical mucosal that lines the endocervical canal, constitutes 1 to 2% of total extrauterine pregnancy. Few hypothesis about the occurrence of cervical ectopic postulated, possibly due to too rapid transport of the blastocyts through immature endometrium for implantation or late fertilization of the ovum takes place in the endocervical canal. 9 Because of the rare incidence, majority of these cases associated with substandard care secondary to misdiagnosis or under diagnosis, result in life threatening haemorrhage after the “usual” procedure. Cervix is a high vascularised area not only predisposed to implantation of fertilized ovum but also vulnerable to torrential bleed after disruption of mucosal lining. Microscopically, only 20% of cervix consists of smooth muscle, so the majority non contractile fibrous tissue has suboptimal mechanical haemostatic manipulation and is insusceptible responding to uterotonic agent. treatment of CEPs, commonly there are high and low dose preparation. The route of administration can be systemic via intramuscular, local injection into ectopic sac or a combination of both. Sometimes, a local MTX injection can be carried out either by intra-amniotic or intra-cervical administration. If embroyonic cardiac activity is detected, feticide can be performed by intracardiac injection of potassium chloride, intra amniotic instillation MTX or direct traumatic punctures under transvaginal ultrasound guidance by experienced personnel. Exclusive operative method in the past tends to have higher failure rate, about 22% of the cases ended up hysterectomy. Recent review of case series suggests that combination of medical and uterine conservative procedures promote better outcome, with less drastic intervention, but significant improvement in maternal consequences as compared to exclusive operative method.9 More importantly, fertility is preserved in such cases. Mechanical evacuation of CEP is preferably performed by suction curettage than conventional dilatation and curettage which is less bleeding and under better control, in term of avoiding excessive curettage of uterine wall tissue. Sonographic guidance during the procedure helps to ensure adequate removal of trophoblastic tissues at focused point. Haemostasis should be applied towards the end of curettage to prevent further bleeding in view of structural potency for cervical tissue to have extensive haemorrhage. It can be achieved by various means: Local injection of vasopressin or carboprost, cervical cerclage, cervical stay sutures, mechanical compression by uterine cavity tamponade balloon, uterine artery ligation, or embolization of the descending branches of the uterine arteries. 3 Intracervical filtration of vasopressin or carboprost, cervical cerclage and cervical stay sutures theoretically should be planned before the surgical removal of ectopic tissue, after confirmed diagnosis of cervical ectopic.3 Risk of infections, necrosis of bladder or rectum caused by erosion from the suture, uterine infarction and sciatic nerve injury can be occurred. However, a trained person is needed to perform the procedure and it could be difficult if uncontrolled bleeding obscures the anatomical view. Uterine tamponade carries its intermediate role in controlling uterine haemorrhage between less invasive method such as conventional uterine massage and uterotonic drugs and more invasive methods such as uterine compression suture, uterine artery ligation and arterial embolisation, before decision of hysterectomy. It seldom acts as monotherapy in the management of post abortal haemorrhage but has significantly reduced maternal morbidity or mortality when combined with other modalities of treatment. It is widely recognized as one of the life saving measurement in acute uterine bleeding. Concept of uterine tamponade has been introduced since 1980s which was started off with uterine packing in controlling intractable uterine bleeding in postpartum and post abortal uterus. 6, 7 Practically, the mechanism of action is to exert external compression against intrauterine wall to obliterate injured uterine vessel, promote platelet aggregation which release effective vasoconstrictors then allow coagulation to act on time. Meanwhile, regular contraction of smooth muscle maintains uterus in contracted state. Yet, introduction of vaginal pack blindly into uterus can cause intrauterine infection or uterine perforation in vulnerable uterus. Multiple revision and innovation have been ongoing for years, use of various type of hydrostatic balloon catheter has replaced uterine packing nowadays. Condom catheter, Foley’s catheter, Rusch catheter, Bakri balloon, BT balloon and Sengstaken – Blakemore oesophageal tube have been used in several case series that eventually achieve satisfactory haemostasis.5 Use of cervical ripening balloon will be another alternative especially in achieving localized haemostasis in endocervical region. Hydrostatic balloons are preferred as the contour of the balloon adapts the unique configuration of the semi rigid uterine cavity to tamponade uterine bleeding. Use of uterine tamponade device requires minimal training which can be also performed by trained medical staffs, particularly for those originate from low resources setting or without surgical facilities. It has important role in preventing further volume loss during transporting patient to tertiary health centre or while waiting for optimization of patient haemodynamic status before proceed to further invasive procedures. Sometimes, it is known as a ‘test’ in given period of interval to decide whether subsequent intervention is necessary. Concurrent uterotonic agent and tamponade balloon are recommended to serve dual mechanism, which is sustaining the uterus at contracted state and blockage of exposed raw vessels area. There is no clear recommendation about the duration of balloon tamponade should be left in situ, usually is CONCLUSION As in this case, patient’s past surgical history provided vital piece of information, there is high suspicious index of possible cervical pathology after two previous caesarean sections. Her irregular menstrual pattern was unable to provide further information about gestational age. Presumed “incomplete miscarriage” earlier on subjected patient for usual evacuation of retained product of conceptus (POC). Diagnosis was established during laparotomy with direct visualisation of abnormal anterior cervix. Process of resuscitation and stabilization might be difficult if patient developed circulatory collapse without anticipation of extensive haemorrhage before procedure. Haemostasis by vaginal pack did provide short tamponade effect during patient transfer. Use of uterotonic agent may be considered in this case as well. Before retrieval of patient to the tertiary hospital, pre-transfer resuscitation and stabilisazation are mandatory with large bore intravenous assess and adequate blood product to standby before proceeding for major operation. In view of disruption of ectopic sac by previous curettage and high vascularised cervical canal post cervical implantation, gentle suction and curettage was performed under ultrasound guidance to evacuate as much conceptus as possible by focusing on the exact implantation site. Ideally, Doppler ultrasound will be helpful in that situation. Previous uterine surgery again increases the possibility of adherent product of conceptus which makes full evacuation hazardous. In this case, minimal POC is felt adherent after suction curettage at anterior endocervix. The tamponade method in this case is achieved by insertion of Bakri balloon under ultrasound guidance. The design of Bakri balloon carries few advantages as it follows the contour of the uterine cavity and silicone material causes less allergic reaction as compare to traditional latex material. Cervical ripening balloon is another better choice as it anchores around cervical region. Single dose of intramuscular MTX was given for the patient after procedure to regress the remaining trophoblastic tissue. She recovered well after the procedure, Bakri balloon was removed with caution after 24 hours in situ without recurrent bleeding reported. Patient was under close follow up for her serum beta hCG monitoring after discharge from hospital, with initial post operative reading 650 mIU/ml decrease to 1.3 mIU/ml after 2 weeks. There is no standardized protocol in management of cervical ectopic pregnancy. In general, successful treatment of CEP can be achieved by means of surgical curettage followed by adequate local haemostasis and use of systemic methotrexate.7, 9 Successful haemostasis is the main modality to avoid hysterectomy. Balloon tamponade is the common practice among other mode of local haemostasis. Exclusive conservative treatment with methotrexate is reserved for cases fulfilled the defined preconditions. There is still inadequate review about weigh between giving MTX before the curettage procedure or after the procedure. Nevertheless, identification of risk factors and early diagnosis of cervical ectopic pregnancy by mode of transvaginal ultrasound with or without Doppler study is important to plan for subsequent intervention. DIAGNOSIS Historically, CEP diagnosed by retrospective histopathological confirmation after a curettage that complicated by life threatening haemorrhage requiring hysterectomy to save life.1 Recognition of risk factors, detailed clinical examination and use of transvaginal ultrasound imaging assist in early detection of extrauterine pregnancy. Damage of the endometrial lining by previous procedure is the main risk factor for EP, such as previous history of uterine curettage is found in 70% or more CEP1, insertion of intrauterine device (IUD) and in vitro fertilization. Other risk factors include previous caesarean section or pelvic surgery, cervical endometriosis, endomyometritis, Asherman’s syndrome, fibroids, uterine adhesion, history of exposure to diethylstilbestrol, previous infective cervicitis such as gonorrhea or Chlamydia associated with CEPs. 9 Increasing trend of invasive method in ART nowadays contributes to even higher prevalence of CEP. In fact, it is not surprised that CEP is often mistaken as incomplete miscarriage, cervical abortion, prolapsed fibroid, or cervical cancer.8 Clinical presentation of CEP is similar to intrauterine miscarriage: per vaginal bleed associated with abdominal pain. In certain case, urinary symptoms secondary to mechanical irritation or compression of the urethra, maybe found in CEP other than other site of EPs. Vaginal examination might reveal enlarged, bulging and extended cervix till external cervical os. Transvaginal ultrasound is main diagnostic tool in identifying more than 80% of CEPs.2 There are some sonographic features that helps to distinguish CEP from other miscarriage in progress: empty uterus with “hour-glassed” appearance, detected gestational sac below the uterine arteries with increased Doppler blood flow around the gestational sac and opened external os but internal os is closed. There is absence of “sliding sign” in CEP upon pressure applied by ultrasound probe. This helps to differentiate from intrauterine pregnancy which is in the process of aborting through the cervix. Transvaginal cervical ectopic sac with yolk sac Transvaginal cervical ectopic MANAGEMENT In 1980’s, hysterectomy is commonly performed to save patient’s life when extensive bleeding occur during dilatation and curettage for a presumed incomplete miscarriage in the actual case of CEPs.1 Nowadays, collaboration of different entity of management help to preserve patient’s fertility, especially for low parity young patients. Management of CEPs comprises of three major principles: systemic or local application of methotrexate, mechanical termination of ectopic sac by curettage and haemostasis via pharmacological, mechanical or operative procedure. Haemostasis is the most vital component to determine whether the patient requires hysterectomy. Expectant management is only applicable for patients who are haemodynamically stable and asymptomatic during the first presentation, with the initial serum beta hCG less than 1000 mIU/ml. About 88% of patients have successful outcome. This is provided no sonographic visualization of an ectopic gestation sac and the serial control serum beta hCG shows reducing trend. Spontaneous abortion of cervical ectopic pregnancy is also possible but rare. Methotrexate (MTX) is a folic acid antagonist, which inhibits DNA synthesis in rapidly growing trophoblastic cells in cervical ectopic. No standardized protocol available for MTX regimen in REFERENCES Starita A, Di Miscia A. Cervical ectopic pregnancy: clinical review. Clin Exp Obstet Gynecol. 2006; 33(1): 47-9 Mohammad R. Mohebbi, Kurt A. Rosenkrans, Eric E. Luebbert. Ectopic Pregnancy in the Cervix: A Case Report. Case Reports in Medicine, Vol 2011, Article ID 858241, 2 pages De La Vega GA, Avery C, Nemiroff R, Marchiano D. Treatment of Early Cervical Pregnancy with Cerclage, Carboprost, Curettage, and Balloon Tamponade. Obstet Gynecol. 2007 Feb; 109 (2 Pt2): 505 – 7 Verma U, Goharkhav N. Conservative management of cervical ectopic Pregnancy. Fertil steril. 2009 Marc, 91 (3): 67-4. Epub 2008 Mar 12 Royal College of Obstetricians and Gyanecologists. Prevention and Management of Postpartum haemorrhage. Green-top Guideline No.52 May 2009 Goldrath MH. Uterine Tamponade for the control of acute uterine bleeding. AMJ Obstet Gyneco 1983 Dec 15; 147 (8): 869-72 Haq G. et al. Control of postpartum and post abortal haemorrhage with uterine packing. J Pak Med Assoc. 2005 Sep; 55 (9): 369-71 Jaime Rosenzweig, MD and Robert H. Birkhan, MD. Cervical ectopic pregnancy Case Report: Findings for the Bedside sonographer. The Journal of Emergency Medicine, Vol. 36, No.1 pp.34-36, 2009 Friederike Hoellen, MD; Klaus Diedrich, MD; Christine Dittmer, MD. Cervical Ectopic Pregnancy: Therapeutic Management. Expert Review of Obstetrics & Gynecology. 2011;6(1):91-98 Left: Transabdominal view of uterus after suction curretage for cervical ectopic Right: Post inflation of Bakri balloon at endocervical region with 60cc of normal saline at ectopic site, uterine fundus is empty Bakri Tamponade Balloon Catheter Cervical Ripening Balloon