Download
1 / 32
320 likes | 333 Views
Explore the role of PPAR activation in reducing cardiovascular risk through genetic background, food intake, obesity, and more. Learn about PPAR isotypes, their modulation, and implications in atherosclerosis. Discover PPAR-γ activation benefits on insulin sensitivity, dyslipidemia, and CV health. Get insights into PPAR-γ modulators and their impact on metabolic processes and inflammation. Uncover how PPAR-γ activation can prevent diabetes, improve β-cell function, and reduce cardiovascular risk factors.

E N D
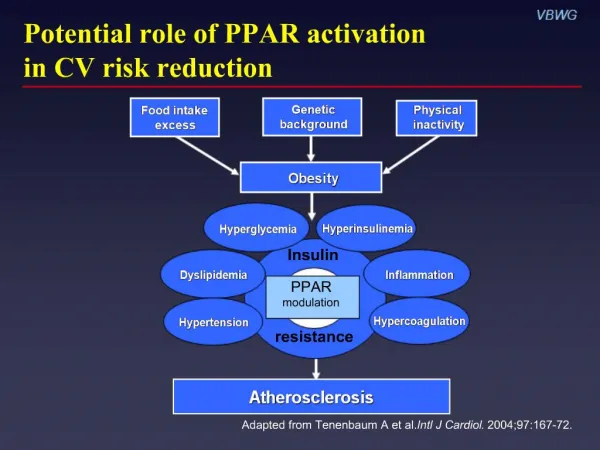
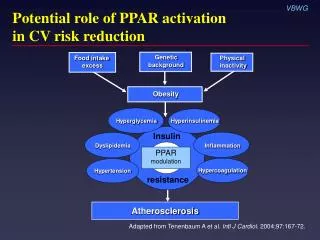
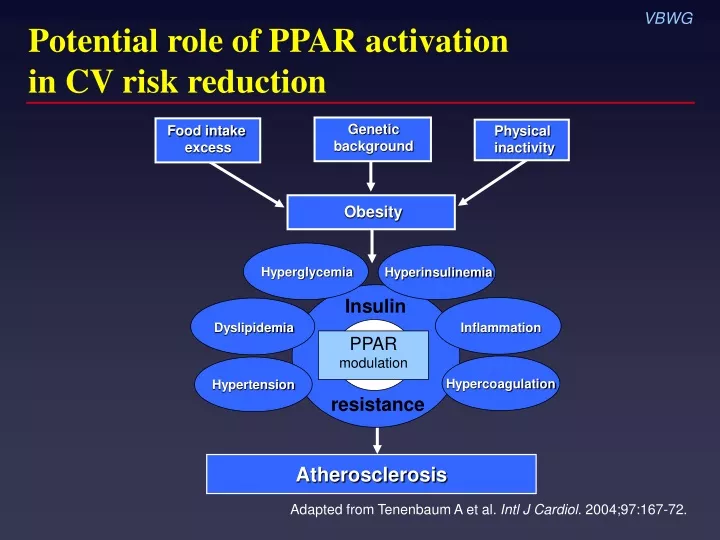
Potential role of PPAR activation in CV risk reduction Geneticbackground Food intake excess Physical inactivity Obesity Hyperglycemia Hyperinsulinemia Insulin Dyslipidemia Inflammation PPAR modulation Hypercoagulation Hypertension resistance Atherosclerosis Adapted from Tenenbaum A et al. Intl J Cardiol. 2004;97:167-72.
Peroxisome proliferator-activator receptors (PPARs): Overview • Family of steroid hormone nuclear receptors • Three isotypes identified • PPAR • PPAR • PPAR • Ligand-activated transcription factors regulatingmetabolic processes Plutzky J. Science. 2003;302:406-7.
PPAR activation and atherosclerosis: A hypothesis Ligandendogenous or synthetic Activated PPAR receptor DirectVascular and inflammatory cells IndirectFat, liver, skeletal muscle Cytokines Chemokines Cholesterol efflux Adhesion molecules FFA Glucose Insulin sensitivity Triglycerides HDL Reducesinflammation ? ? ? ? Blunts atherosclerosis Adapted from Plutzky J. Science. 2003;302:406-7.
Focus on PPAR activation • Reduces insulin resistance • Preserves pancreatic -cell function • Improves CV risk profile Improves dyslipidemia ( HDL, LDL density, or TG) Renal microalbumin excretion Blood pressure VSMC proliferation/migration in arterial wall PAI-1 levels C-reactive protein levels Adiponectin Free fatty acids Inzucchi SE. JAMA. 2002;287:360-72.
PPAR modulators Name Trade name Manufacturer Approval status Troglitazone Rezulin Parke-Davis 1997* Rosiglitazone† Avandia GlaxoSmithKline 1999 Pioglitazone‡ Actos Eli Lilly/ 1999 Takeda Pharmaceuticals Muraglitazar§ Pargluva Bristol-Myers Squibb/ NDA Merck submitted 2004 *Withdrawn March 2000 †Also available in combination with metformin or sulfonylurea ‡ Also available in combination with metformin§Dual PPAR/ agonist
PPAR modulation: Newest strategy in CV risk reduction Hyperinsulinemia Hyperglycemia Insulin Dyslipidemia Inflammation PPAR modulation Hypercoagulation Hypertension resistance Adapted from Tenenbaum A et al. Intl J Cardiol. 2004;97:167-72.
Factors that may drive the progressive decline of -cell function Insulinresistance Hyperglycemia (glucose toxicity) -cell “Lipotoxicity” (elevated FFA, TG) Adapted from Kahn SE. J Clin Endocrinol Metab. 2001;86:4047-58. Adapted from Ludwig DS. JAMA. 2002;287:2414-23.
TRIPOD: Evidence that insulin resistance causes -cell failure N = 266 Hispanic women with gestational diabetes randomized to troglitazone 400 mg or placebo for median 30 months • PPAR activation: 55% relative risk reduction for new-onset diabetes (HR 0.45; 0.25–0.83) • Effect was most prominent in women with initial increase in insulin sensitivity and accompanying large reduction in insulin output • Protection persisted 8 months after cessation of active treatment • PPAR activation associated with preserved -cell function TRIPOD = Troglitazone in Prevention of Diabetes Buchanan TA et al. Diabetes. 2002;51:2796-803.
DPP: Improving insulin sensitivity/secretion prevents diabetes 30 Placebo Metformin Lifestyle Insulinsecretion(IGR) 25 20 Low Medium 15 High 10 5 Insulinsecretion(IGR) 0 High Low Medium Low Medium High Low Medium High Insulin sensitivity (1/fasting insulin) N = 3234 Diabetes hazard rate (per 100 pyr) pyr = person years IGR = insulin-to-glucose ratio DPP = Diabetes Prevention Program DPP Research Group. Diabetes. 2005;54:2404-14.
PPAR activation blunts progression to diabetes Diabetes Prevention Program 15 Placebo Metformin 850 mg 10 Cumulative incidence (%) Lifestyle Troglitazone400 mg* 75% vs placeboP < 0.001 5 0 0.0 0.5 1.0 1.5 Years n = 2343 1568 237 739 DPP Research Group. Diabetes. 2005;54:1150-6. *Terminated early after 1.5 years
PPAR activation improves -cell function N = 17 with type 2 diabetes 5 P = 0.02 4 3 Disposition index 2 1 0 Rosiglitazone 8 mg Insulin –1 Acute insulin response to glucose (µIU/mL/10 min) Disposition index = HOMA-IR HOMA-IR = Homeostasis model assessment of insulin resistance Ovalle F, Bell DSH. Diabetes Care. 2004;27:2585-9.
CV implications of insulin resistance and PPAR activation Hyperglycemia Hyperinsulinemia Insulin Dyslipidemia Dyslipidemia Inflammation PPAR modulation Hypercoagulation Hypertension resistance Adapted from Tenenbaum A et al. Intl J Cardiol. 2004;97:167-72.
Importance of LDL particle density • In insulin resistance, LDL-C levels are similar or only slightly elevated vs general population • However, atherogenicity of LDL particles varies according to density – More dense = more atherogenic • Proportion of small, dense LDL particles greater in patients with insulin resistance or diabetes vs general population Miranda PJ et al. Am Heart J. 2005;149:33-45.
Greater atherogenicity of small, dense LDL vs normal LDL Susceptible to oxidation Binds to arterial wallPenetrates arterial wall Toxic to endothelial cells Promotes PAI-1 production by endothelial cellsPromotes thromboxane production by endothelial cellsAccumulates Ca2+ in vascular smooth muscle cellsBinds to LDL scavenger receptor Adapted from Sniderman AD et al. Ann Intern Med. 2001;135:447-59.
Increased small, dense, LDL particles associated with reduced IHD survival N = 2072 men without IHD at baseline;13-year follow-up 1.00 Survivalprobabilities 0.90 P < 0.001 0.80 0 2 4 6 8 10 12 Follow-up (years) Tertiles of LDL-C255Å 1.07–1.86 mmol/l ≥1.86 mmol/l <1.07 mmol/l St-Pierre AC et al. Arterioscler Thromb Vasc Biol. 2005;25:553-9. IHD = ischemic heart disease
PPAR activation increases LDL size and buoyancy N = 302; rosiglitazone 8 mg LDL density LDL particle size 0.04 8 P < 0.0001 P < 0.0001 Relativeflotationvs baseline Diametervs baseline(Angstroms) 4.8 0.019 4 0.02 0 0 Brunzell JD et al. Circulation. 2004;110(suppl):III-143.
Comparative effects of PPAR activators on lipids in diabetes • In patients not receiving statin therapy, studies suggest that pioglitazone and rosiglitazone have differing effects on lipid levels and particle size1 • In patients receiving statin therapy, some studies suggest these differences are eliminated, while other studies suggest they persist2 • Clinical implications are not known3 1Goldberg RB et al. Diabetes Care. 2005;28:1547-54. 2Plotkin DJ et al. Diabetes. 2005;54(suppl 1):A232. 3Khan M et al. Diabetes. 2005;54(suppl 1):A137.
CV implications of insulin resistance and PPAR activation Hyperglycemia Hyperinsulinemia Insulin Inflammation Inflammation Dyslipidemia PPAR modulation Hypertension Hypercoagulation resistance Adapted from Tenenbaum A et al. Intl J Cardiol. 2004;97:167-72.
Adipokines: An overview CRP IL-6 PAI-1 Angiotensinogen Leptin Resistin MCP-1 Adiponectin Antiatherogenic Atherogenic Lau DCW et al. Am J Physiol Heart Circ Physiol. 2005;288:H2031-41. Wellen KE, Hotamisligil GS. J Clin Invest. 2005;115:1111-9.
Adiponectin associated with decreased risk of MI N = 18,225 men; 6-year follow-up 1.2 1.0 0.8 Relative 0.6 risk 0.4 0.2 0.0 1 2 3 4 5 Quintile of adiponectin (95% CI) g/mL 7.9 12.6 16.5 21.1 29.2 m Adjusted relative risk (P < 0.001) Lipid-adjusted relative risk (P < 0.02) Pischon T et al. JAMA . 2004;291:1730-7.
Improved insulin sensitivity associated with increased adiponectin N = 40 women with gestational diabetes treated with troglitazone for 3 months 500 400 % Change in insulin sensitivity (Si) 300 200 100 –50 –25 25 50 75 100 –100 % Change in HMW/total adiponectin (SA) Pajvani UB et al. J Biol Chem. 2004;279:12152-62.
Contrasting roles of CRP and PPAR on inflammation and insulin resistance Adipose tissue IL-6 Liver CRP PPAR Glucose Insulinresistance Lau DCW et al. Am J Physiol Heart Circ Physiol. 2005;288:H2031-41.
Direct relationship of CRP to metabolic syndrome Women’s Health Study; N = 14,719 8 6 Median CRP(mg/L) 4 2 0 0 1 2 3 4 5 Components of the metabolic syndrome (n) n = 4086 3884 3152 2292 1135 170 Ridker PM et al. Circulation. 2003;107:391-7. Modified ATP III definition
Inflammation is a contributing mechanism in diabetes development N = 1047 25 20 P = 0.06 P = 0.001 P = 0.001 Incidence(%) 15 10 5 0 Fibrinogen CRP PAI-1 Quartiles of inflammatory proteins 1st 2nd 4th 3rd Festa A et al. Diabetes. 2002;51:1131-7.
PPAR activation decreases CRP in patients with diabetes N = 357; 26 weeks Rosiglitazone 4 mg Rosiglitazone 8 mg Placebo 0 –10 Mean change from baseline(%) –20 –30 –40 P < 0.05 –50 27% P < 0.05 22% Haffner SM et al. Circulation. 2002;106:679-84.
CV implications of insulin resistance and PPAR activation Hyperglycemia Hyperinsulinemia Insulin Dyslipidemia Inflammation PPAR modulation Hypercoagulation Hypertension Hypertension resistance Adapted from Tenenbaum A et al. Intl J Cardiol. 2004;97:167-72.
Improved insulin sensitivity associated with reduced BP VBWG N = 24 nondiabetic hypertensives; rosiglitazone 8 mg, 16 weeks 20 10 in 24-h systolic BP(mm Hg) 0 –10 –20 –2 –1 0 1 2 3 Change in insulin sensitivity (mg/kg/min) Low-renin hypertension Nonmodulators P < 0.005r = –0.59 Raji A et al. Diabetes Care. 2003;26:172-8.
PPAR activation associated with sustained BP reduction N = 668 with type 2 diabetes Rosiglitazone added to baseline therapy Baseline metformin 6 months 12 months Baseline sulfonylurea 6 months 12 months –6 –5 –4 –3 –2 –1 0 1 –5 –4 –3 –2 –1 0 1 24-h diastolic BP*Treatment differences (mm Hg, 95% CI) 24-h systolic BP*Reduction from baseline (mm Hg, 95% CI) *Ambulatory BP Home PD et al. Diabetes. 2005;54(suppl 1):A134.
CV implications of insulin resistance and PPAR activation Hyperglycemia Hyperinsulinemia Insulin Dyslipidemia Inflammation PPAR modulation Hypercoagulation Hypertension resistance Adapted from Tenenbaum A et al. Intl J Cardiol. 2004;97:167-72.
PPAR activation blunts TNF-–induced PAI-1 secretion Human umbilical-vein endothelial cells 800 600 PAI-1 (ng) 400 † 200 * * 0 TNF-1 ng/mL+Trog 10 µM TNF-10 ng/mL TNF- 10 ng/mL +Trog 10 µM TNF-100 ng/mL TNF-1 ng/mL TNF- 100 ng/mL +Trog 10 µM Trog = troglitazone *P < 0.001 †P < 0.005 Hamaguchi E et al. J Pharmacol Exp Ther. 2003;307:987-94.
Metformin reduces PAI-1 levels in type 2 diabetes N = 27, 12 weeks 35 30 25 20 15 10 5 0 PAI-1 activity(U/mL) * Basal Placebo Metformin 2.5 g Results at 12 weeks A1C= –1.3% FPG = –55 mg/dL Nagi DK, Yudkin JS. Diabetes Care. 1993;16:621-9. * P = 0.001 vs placebo
Benefits of combined insulin sensitizer therapy: Effects on CRP, PAl-1, and MMP-9 Weeks 8–24 MMP-9 30 * 22.2 20 10 Baseline(%) CRP PAl-1 0 –0.56 –10 –9.8 –14.35 * –20 P = 0.046 –30 –26.9 –32.76 P = 0.026 –40 P < 0.001 Metformin 2 g (n = 70) Metformin 1 g + rosiglitazone 8 mg (n = 57) Weissman PN et al. Diabetes. 2004;53(suppl 2):A28. *NS vs baseline