Download
1 / 36
360 likes | 519 Views
Control number: 1054 Session : 127. All of the authors of this presentation do not have any financial interest or other relationships with any commercial products or services discussed in the exhibit. VIRTUAL INTRAVASCULAR MR ENDOSCOPYC EVALUATION OF CEREBRAL ANEURYSM S.

E N D
Control number: 1054 Session : 127
All of the authors of this presentation do not have any financial interest or other relationships with any commercial products or services discussed in the exhibit.
VIRTUAL INTRAVASCULAR MR ENDOSCOPYC EVALUATION OF CEREBRAL ANEURYSMS Incesu, L. Erenler, CZ. Tokatlıoglu, O. Yildirim, O. Taskin, G. Akan, H. Diren, B ONDOKUZ MAYIS UNIVERSITY, SAMSUN, TURKEY
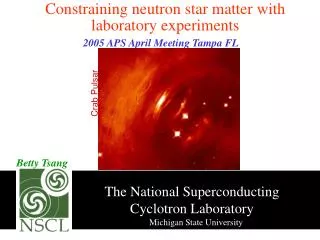
Recent advances in MR and CT made it possible to provide high resolution images with near isotropic voxels. In addition, various rendering techniques have produced good contrast between the objects and the surrounding structures. These new technologies have made it possible to produce virtual MR and CT endoscopy which can be applied for visualization of the vascular spaces.
Virtual endoscopy is a terminology used to describe a new method of image display using computer processing of 3D data sets to provide simulated visualization of patients hollow organs similar to that produced by standard endoscopy. A perspective volume rendering method is used and volume data are rendered from a point source at a finite distance to approximate the human visual system with the use of virtual endoscopic algorithm.
The virtual endoscopic images can demonstrate to the viewer smooth or uneven inner surfaces of the vessels such as protrusions or depressions because of the shading. With a virtual endoscopy, a closer object appears larger than an object of identical size at a greater distance from the viewer. MR endoscopy were routinely used for the large abdominal and thoracic vessels, however, studies regarding it’s use in the intracranial applications are limited.
PURPOSE Correct determination of the morphology, exact size and inside of the aneurysm, and it’s relation to the parent artery increases the success of surgery or endovascular treatment. Multidetector CT angiography (CTA) and magnetic resonance angiography (MRA) are the routine imaging methods used in the diagnosis of cerebral aneurysm . According to our knowledge, this is the first study where the virtual intravascular endoscopy is used in the evaluation of aneurysm.
MATERIAL & METHODS Sixteen channel MD-CTA and 3D TOF MRA examinations were performed in patients who suspected to have cerebral aneurysm. DSA examination were performed in certain patients when required. 3D TOF MRA data were transferred to a workstation computer system. Virtual intravascular MR endoscopy technique were used on MRA maximum intensity projection (MIP) images.
Virtual Endoscopy After an image data set was loaded, axial, coronal, and sagittal sections, as well as endoscopic view, were presented on the screen. Images in three plans helped the operator orient to the anatomy depicted on the 3D display and steer the endoscopic view via fly through. Threshold value (low 0 - high 200) were selected for surface shaded display.
Application of virtual intravascular MR endoscopy to 3D TOF MIP images
Using fly through technique, the presence of aneurysm, size of the neck , whether thrombus is present and the inner surface texture of aneurysm were evaluated by moving inside vessels related to aneurysm.
RESULTS Age Thirty patients ranging between 12 and 75 years (mean age 52,8) of whom 12 were male and 18 were female, were included in the study. Number A total of 37 aneurysms were detected in 30 patients by the use of CTA and MRA. Twenty two of this patients had subarachnoid hemorrhage (SAH).
Fig. 1.A 75 years old patient with SAH. At MDCTA (a) and images of thin MIP MRA (b) bilateral saccular aneurysms in relation to PCoA were seen one of 7.5 mm in diameter in the left (large arrow), and another of 4 mm in diameter in the right (small arrow). Moving inside the right (c), and left (d) PCoA (thin arrows) of the same patient by virtual endoscopy, the shape, size, andinternal surface texture (thick arrows) of the two different aneurysmal sac were seen.
Location Of the 37 aneurysms 12 were located in anterior communicating artery (ACoA), 9 in middle cerebral artery (MCA) and its bifurcations, 6 in posterior communicating artery (PCoA), 2 in anterior cerebral artery, 2 in posterior cerebral artery (PCA), 2 in internal carotid artery (ICA) and it’s segmental branches, 2 in posterior inferior cerebellar artery (PICA), 1 in ophthalmic artery, and 1 in basilar artery.
Fig. 2. A seventy one years old patient with right 3rd crainal nerve paralysis. MDCTA (a) and thin MIP MRA (b) images showing a saccular aneurysm of 8 mm in diameter at the right PCoA (arrow). Aneurysmal sac (thick arrows) is seen at virtual MR endoscopic image of the same patient acquired by entering PCoA (thin arrows) (c). b a
Size The diameter of two of the aneurysms were 75mm and 25mm (giant aneurysm), whereas the largest of the remaining aneurysms was 11.7 mm, the smallest was 2.2mm. Two of the 37 aneurysms were fusiform in shape, and 11 of the rest 35 saccular aneurysms with wide neck, 24 with narrow neck. Even if the evaluation of the size during operation was not objective, results were similar to CTA and MRA.
Fig. 3. Forty three years old patient with severe headache. MDCTA right inferior oblique (a) and thin MIP MRA images (b) a saccular aneurysm of 2 mm in diameter at the AcoA (arrow) is present. Virtual MR endoscopic image of the same patient (c) left ACA A2 segment (thin arrow) and adjacent to it an aneurysmal sac (thick arrow) is seen.
Thrombus Virtual intravascular MR endoscopy demonstrated thrombus formation in 10 aneurysms, whereas CTA depicted thrombus in only one which was a giant aneurysm. Wall discontinuity In one patient, MR endoscopy demonstrated a focal discontinuity at the posteromedial wall of an aneurysm located at PCoA.
Fig. 4. A sixty years old patient with 3rd cranial nerve paralysis. A posterior superior view of MDCTA (a) and thin MIP MRA (b) images, a saccular aneurysm of 11.7 mm at the right PCoA (thick arrow), and another on of 6.8 mm in diameter at the right MCA bifurcation (thin arrow) are seen. Virtual MR endoscopic image of the same patient acquired by entering to the M2 segment of right MCA (thin arrows) (c) aneurysmal sac (thick arrows) is seen. Whereas endosocpic image acquired by entering to PCoA (thin arrows) (d) aneurysmal sac (thick arrows) with discontinuity at it’s posterior medial wall (arrowhead) is noted.
Fig. 4e. Virtual endoscopic entering to PCoA aneurysm and discontinuity at it’s posterior medial wall
Fig. 5.Fifty two years old patient with severe headache. MDCTA (a) thin MIP MRA (b) images showing a saccular aneurysm of 10.5 mm in diameter at the right ophthalmic artery. Virtual MR endoscopic image of the same patient ( c) showing the lumen of supraclinoid segment of ICA(thin arrows), aneurysmal sac (thick arrow) , and thrombus formation inside the aneurysm (thick arrows) are noted.
Fig. 5d.Virtual endoscopy of thrombus which almost filled the lumen is passed by force
Lobulation and Perforant Artery • Virtual endoscopy also gives us useful • informations in some patients about • aneurysmal lobulation and whether perforant • artery is present.
Fig.6. A perforant artery is seen at thin MIP (a) and at virtual endoscopy (b), the aneurysm has a trilobulated dome where the perforating artery arisen from. Notice that the configuration of the dome is well demonstrated at virtual endoscopy . The inside of perforating artery and the neck are better seen by reducing threshold values. a b
Fig. 7. At CTA (a) and virtual endoscopy (b) a bilobulated aneurysm on the bifurcation of MCA with thrombus inside the lumen is demonstrated. a b
Apart from inner surface texture and existence of thrombus, there is no significant difference between CTA and MRA regarding the number, location, size and neck shape of aneurysms.
DISCUSSION In our days, it is possible to image aneurysms noninvasively by using methods such as CTA and MRA. Methods like surface rendering where a window was opened from outside of the aneurysm, were used to visualize it’s internal texture, and to acquire knowledge about the diameter, localization and the neck.
Conditions like tortuous vessel, presence of SAH and vessel spasm make it difficult to evaluate the neck and internal structure of aneurysm by CTA and MRA. Small aneurysms may not be visualized because of adjacent bone at CTA and flow artifact at MRA.
Advantages Virtual MR endoscopy can be easily applied in all arterial MRA examinations. By the use of virtual MR endoscopy, in routine 3D TOF arterial MRA examination it is possible to move inside all of the branches that are demonstrated by MIP. Use of contrast medium doesn’t effect directly virtual endoscopy examination, however, when it is used, the distal branches are visualized . Thus, it is possible to move inside the lumen and endoluminal assessment with navigation.
Limitations The produced images are operator-dependent and the threshold algorithm may change the size and shape of the objects. The image quality of the virtual endoscopy depends on that of source images and rarely signal loss or artifact may prevent entering to the vessel lumen.
CONCLUSION With intravascular virtual MR endoscopy, we can move in slim vessels and small cerebral aneurysms 1-2 mm in diameter, therefore the aneurysm’s relation to parent artery, neck and inside of sac can be evaluated easily. Virtual intravascular MR endoscopy is easy and reliable technique which can be performed to MRA MIP images particularly before interventional procedures.
REFERENCES 1. Grossi G, Romanzi F, Macchia G, Ruffinengo U, Calia S. Angio-CT: a proposal for emergency diagnosis in subarachnoid hemorrhage as a preliminary to therapeutic choices. Intervent Neuroradiol 1995;1:43-57. 2. Hoff DJ, Wallace MC, terBrugge KG, Gentili F. Rotational angiography assessment of cerebral aneurysms. AJNR1994;15:1945-8. 3. Hsiang JNK, Liang EY, Lam JMK, Zhu XL, Poon WS. The role of computed tomographic angiography in the diagnosis of intracranial aneurysms and emergent aneurysm clipping. Neurosurgery1996;38:481-7. 4. Ogawa T, Okudera T, Noguchi K, et al. Cerebral aneurysm: evaluation with three dimensional CT angiography. AJNR1996;17:447-54.
5. Bontozoglou NP, Spanos H, Lasjaunias P, Zarifis G. Intracranial aneurysms: endovascular evaluation with three dimensional-display MR angiography. Radiology1995;197:876-9. 6.Futami K, Mitsutoshi N, Masayuki I et al::Simulation of clipping position of cerebral aneurysms using three-dimensional computed tomography angiography. Neurol Med Chir (Tokyo) 2004:44;6-13. 7. Marro B, Galanaud D, Valery C, et al.: Case Report. Intracranial Aneurysm: Inner View and Neck Identification with CT Angiography Virtual Endoscopy. JCAT 1997:21(4); 587-589. 8. Vining DJ. Virtual endoscopy: is it reality? Radiology1996;200:30-1. 9. Kato Y, Sano H, Katada K, et al.: Clinical usefulness of 3-D CT endoscopic imaging of cerebral aneurysms. Neurol Res. 1996;18(2):98-102.