Download
1 / 20
200 likes | 380 Views
Marijuana. CANNABIS SPECIES. Cannabis sativa grows worldwide Tall plant with long, thin light green leaves used for fibers to make cloth and rope, but also used for psychoactive properties. Cannabis indica Plentiful in Mideast, India, and Central Asia Short plant with broad dark leaves

E N D
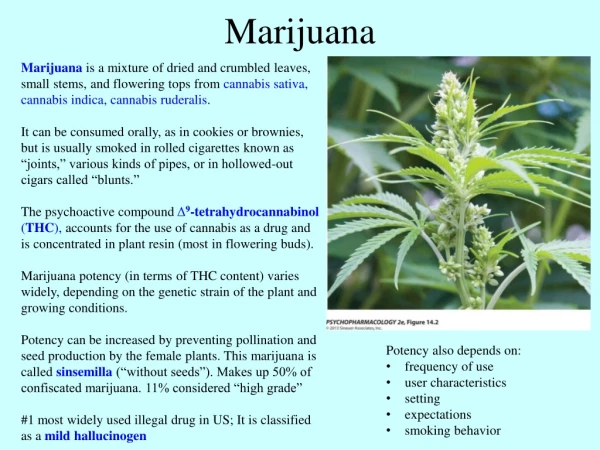
CANNABIS SPECIES • Cannabis sativa • grows worldwide • Tall plant with long, thin light green leaves • used for fibers to make cloth and rope, but also used for psychoactive properties. • Cannabis indica • Plentiful in Mideast, India, and Central Asia • Short plant with broad dark leaves • Mainly used for psychoactive resins. • Cannabis ruderalis • grows primarily in Eastern Europe (Russia, Poland) • Short weedy plant, less THC content than others
CANNABIS • Primary psychoactive agent in Cannabis • delta-9-tetrahydrocannabinol (THC) • Various preparations from Cannabis • Charas (in India) or Hashish • the pure resin from the leaves and stems • avg. concentration of THC is 3% to 7%, as high as 20% • Ganja (in India) or Sinsemilla (Spanish, without seeds) • dried tops of female plants (without seeds) • THC concentration 7 – 12% • Bhang • dried, ground up remainder of the plant • avg. concentration of THC is 1% to 2%
Early History of Cannabis • Cannabis probably originated in central Asia • Cultivated and widely dispersed before recorded history. • Scythians were probably responsible for spreading its use to Egypt and north to Europe and Russia. • In China, Cannabis probably known since ~4000 B.C. • Cultivated for fiber, seed, as well as intoxicating and medicinal properties. • Social use began in North Africa by ~1000 A.D.
Recent History of Cannabis Use • Widespread industrial use of hemp in western Europe and American colonies • psychoactive properties not widely recognized until 19th century • 19th Century: Romantic Literature and the New Science of Psychology • Use expanded into Europe and was widespread among artists and writers. • The new science of psychology also introduced the use and study of psychoactive agents.
HISTORY • “Marijuana, Assassin of Youth” • Sensationalized stories in the news media • e.g., blaming marijuana for violent crimes • 36 states in U.S. had laws regulating the use, sale and/or possession of marijuana by 1935. • The Marijuana Tax Act of 1937 • Did not outlaw Cannabis, but taxed it • After the Marijuana Tax Act • New York Academy study showed no physical or mental deterioration with long-term use.
PHARMACOLOGY • Cannabinoid Chemicals • Over 400 chemicals in marijuana • 61 unique to the cannabis plant • called cannabinoids • Pharmacokinetics • THC is a weak acid with a pKa of 10.6 • not ionized at pH of bodily fluids • When smoked, rapid absorption • Peak effects within 5-10 min. • When ingested, peak effects ~90 min. • Half-life ~ 19 hours, longer for metabolites (20-30 hrs) • Main metabolite: 11-hydroxy-delta-9-THC, which may be more active than delta-9-THC
NEUROPHARMACOLOGY • Mechanisms of Action • CB receptors discovered in brain, 1990 • CB1 receptors: in CNS • primarily in cortex, hippocampus, cerebellum, basal ganglia • CB2 receptors: spleen, immune system • Endocannabinoids were discovered soon after . • Anandamide, 2-arachidonylglycerol (2-AG) • Neuromodulators of multiple neurotransmitters, including monoamines, GABA, ACh and endorphins • Signaling between postsynaptic and presynaptic cells • Interactions with opioid peptides to modulate DA transmission in mesolimbic structures
Acute Physiological Effects • Cardiovascular and Peripheral Effects • Increased heart rate • Variable effects on blood pressure • Dry mouth, “bloodshot” eyes • Effects on Sleep • Drowsiness, increased sleep time • High doses can produce insomnia.
Cognitive/Behavioral Effects • Low to moderate doses produce euphoria, a pleasant state of relaxation, laughter • Some loss of coordination and balance • Simple reaction times relatively unaffected • Complex and choice reaction time, accuracy but not speed affected. • Impaired short-term memory • Reduced sustained attention • Impaired visuo-spatial and temporal processing
Adverse Behavioral Effects • Moderate to high doses may produce mild anxiety to panic and paranoia • A few rare cases have been reported of cannabis-induced psychoses, delusional and bizarre behavior, and hallucinations • These reactions occur most frequently in individuals who are under stress, anxious, depressed or borderline schizophrenic.
Driving Performance • The ability to perform complex tasks, such as driving, may be impaired while under the influence of marijuana. • Laboratory studies with non-regular marijuana users show significant impairments. • Results suggest that marijuana has little effect on ability to control a car, but impairs the driver’s ability to attend to peripheral stimuli. • Effects of THC on driving ability are amplified when combined with alcohol.
Critical Thinking Skills • Marijuana has been found to have a negative impact on critical thinking skills. • Impairment can affect: attention, memory, learning. • An unresolved question is whether these impairments are due to acute drug effects or long-term consequences of regular use.
Behavioral Effects in Nonhumans • Unconditioned Behavior • Biphasic effect on motor activity; initial increase, then depressant effects. • Stimulatory effects represent an exaggerated response to environmental stimuli. • High doses produce ataxia. • Reduced aggressive behavior • Conditioned Behavior • Interference with tasks that assess short term memory • THC decreases avoidance responding, like depressants • Unlike depressants, THC does not increase punished behavior.
Behavioral Effects in Nonhumans • Drug Discrimination • Rats readily learn to discriminate THC • Some evidence for partial generalization to depressants, but not to any other drug classes • THC discrimination is blocked by CB1 antagonists. • Self-Administration • Due to low solubility in water, I.V. self-administration of THC has been difficult to study. • Water soluble synthetic cannabinoids are self-administered. • THC also establishes Conditioned Place Preference in rats.
Health Risks • Abuse/Dependence Potential • Tolerance occurs when high levels are used over long periods. • Physical dependence has been observed under certain heavy use conditions. • Psychological dependence does not occur for most users, but can occur with frequent heavy use. • Withdrawal symptoms occur within 1 day and persist 4-12 days • Anxiety, restlessness, depression, irritability, disrupted sleep, decreased food intake, sometimes increased aggression
Health Risks • Chronic Lung Exposure • Similar chemicals to tobacco • Levels of exposure differ from tobacco • Marijuana as a causal factor in COPD or lung cancer is still debated • Reproductive Effects • Effects noted but significance not known • Immune System Effects • No relationship established between marijuana use and overall death rate
MEDICAL USES OF CANNABIS • China • First mention in 2737 B.C. was medical use • Cannabis mixed with wine was used for anesthetic 2900 years later (A.D. 200) • Europe • Almost no mention until 1800s • 1839, W.B. O’Shaughnessy reported on anticonvulsant and appetite stimulant effects. • Several publications followed regarding numerous other medical uses (e.g., tetanus, neuralgia, dysmenorrhea, asthma, gonorrhea, migraine, alcohol addiction).
MEDICAL USE OF CANNABIS • United States • Some early medicinal use in 1800s • Minimal uses until Marijuana Tax Act of 1937 resulted in withdrawal of existing products • Renewed interest following a 1972 report showed help for glaucoma patient and a 1975 report noted reduced nausea in chemotherapy patients.
MEDICAL USE OF CANNABIS • Suggested medical uses of marijuana include • Reduced intraocular pressure • Antiemetic • Appetite stimulant • Pain management • Reduced muscle spasticity • Recent developments with synthetic derivatives of THC (e.g., Marinol) and oral preparations from cannabis extracts (e.g., Savitex).