Download
1 / 26
260 likes | 328 Views
Explore and compare the study designs, risk factors, statistical methods, and safety evaluations of the RE-LY and ROCKET AF trials in atrial fibrillation management. Understand the definitions of stroke and systemic embolism in each trial to gain insights into their efficacy and safety profiles.

E N D
A Comparison of RE-LY and ROCKET AFTrial Designs and Outcomes C. Michael Gibson, M.S., MD.
RE-LY: Study Design • Patients were eligible if they had atrial fibrillation documented on electrocardiography performed at screening or within 6 months beforehand and at least one of the following characteristics: • Previous stroke or transient ischemic attack • a left ventricular ejection fraction of less than 40% • New York Heart Association class II or higher heart-failure symptoms within 6 months before screening • An age of at least 75 years or an age of 65 to 74 years plus diabetes mellitus, hypertension, or coronary artery disease. Atrial fibrillation ≥1 Risk Factor Absence of contra-indications 951 centers in 44 countries Blinded Event Adjudication. R Open Blinded Dabigatran Etexilate 150 mg BID N=6000 Warfarin adjusted (INR 2.0-3.0) N=6000 Dabigatran Etexilate 110 mg BID N=6000 Connolly SJ, et al. N Engl J Med. 2009;361:1139-1151
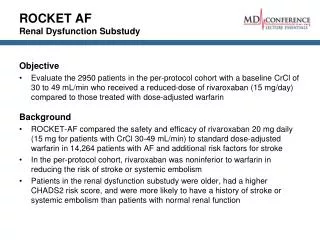
Risk Factors • CHF • Hypertension • Age 75 • Diabetes • OR • Stroke, TIA or Systemic embolus Rocket AF Study Design At least 2 or 3 required* Atrial Fibrillation Rivaroxaban Warfarin Randomize Double Blind / Double Dummy (n ~ 14,000) 20 mg daily 15 mg for Cr Cl 30-49 ml/min INR target - 2.5 (2.0-3.0 inclusive) Monthly Monitoring Adherence to standard of care guidelines Primary Endpoint: Stroke or non-CNS Systemic Embolism * Enrollment of patients without prior Stroke, TIA or systemic embolism and only 2 factors capped at 10% Rocket AF Investigators, AHA 2010
Comparison of Study Designs • Both had non-inferiority to warfarin as primary endpoint • Rocket AF required 2 risk factors for entry, RE-LY 1 risk factor • Rocket AF capped CHADS2 = 2 early in the trial unless a patient scored two points by having a prior stroke/TIA. This may account for the high rate of prior stroke in Rocket AF. • Both randomized trials • Rocket AF administered warfarin in a blinded fashion, RE-LY did not • There was a dose adjustment for impaired CrCl in Rocket AF • INR target range 2-3 in both C. Michael Gibson, M.S., M.D. Rocket AF Investigators, AHA 2010; Connolly SJ, et al. N Engl J Med. 2009;361:1139-1151
Comparison of Study Designs in Other Trials C. Michael Gibson, M.S., M.D. Rocket AF Investigators, AHA 2010; Connolly SJ, et al. N Engl J Med. 2009;361:1139-1151
Statistical Methods: Efficacy RELY: Primary Efficacy Evaluation: Stroke or non-CNS Embolism • Non-Inferiority: Intention-to-treat • Superiority: Intention-to-treat Rocket AF: Primary Efficacy Evaluation: Stroke or non-CNS Embolism • Non-Inferiority: Protocol Compliant on treatment • Superiority: On Treatment, then by Intent-to- Treat RE-LY used Intention to treat for both non-inferiority and superiority testing; Rocket AF used on treatment analysis for first tests of non-inferiority and superiority C. Michael Gibson, M.S., M.D. Rocket AF Investigators, AHA 2010; Connolly SJ, et al. N Engl J Med. 2009;361:1139-1151
Statistical Methods: Safety RELY: • Primary Safety Evaluation: Major bleeding Rocket AF: • Primary Safety Evaluation: Major or non-Major Clinically Relevant Bleeding C. Michael Gibson, M.S., M.D. Rocket AF Investigators, AHA 2010; Connolly SJ, et al. N Engl J Med. 2009;361:1139-1151
RE-LY Definitions of Stroke • Stroke was defined as the sudden onset of a focal neurologic deficit in a location consistent with the territory of a major cerebral artery and categorized as ischemic, hemorrhagic, or unspecified. • Hemorrhagic transformation of ischemic stroke was not considered to be hemorrhagic stroke. • Intracranial hemorrhage consisted of hemorrhagic stroke and subdural or subarachnoid hemorrhage. • Systemic embolism was defined as an acute vascular occlusion of an extremity or organ, documented by means of imaging, surgery, or autopsy. C. Michael Gibson, M.S., M.D. Rocket AF Investigators, AHA 2010; Connolly SJ, et al. N Engl J Med. 2009;361:1139-1151
Rocket AF Definitions of Stroke • The primary efficacy outcome is the composite of stroke • Stroke is defined as a new, sudden, focal neurological deficit resulting from a presumed cerebrovascular cause that is not reversible within 24 hours and not due to a readily identifiable cause such as a tumor or seizure • All strokes will be classified as primary ischemic or primary hemorrhagic • And non-CNS systemic embolism • Non-CNS systemic embolism is defined as abrupt vascular insufficiency associated with clinical or radiological evidence of arterial occlusion in the absence of other likely mechanisms, (e.g., trauma, atherosclerosis, instrumentation) C. Michael Gibson, M.S., M.D. Rocket AF Investigators, AHA 2010; Connolly SJ, et al. N Engl J Med. 2009;361:1139-1151
RE-LY: Baseline Characteristics C. Michael Gibson, M.S., M.D. Rocket AF Investigators, AHA 2010; Connolly SJ, et al. N Engl J Med. 2009;361:1139-1151
Rocket AF: Baseline Demographics Based on Intention-to-Treat Population C. Michael Gibson, M.S., M.D. Rocket AF Investigators, AHA 2010; Connolly SJ, et al. N Engl J Med. 2009;361:1139-1151
Rocket AF was a Higher Risk Patient Population • Whereas 32.4% of patients in RE-LY were low risk CHADS 0-1, there were none of these patients in Rocket AF • Whereas just over 32% of patients in RE-LY were high risk CHADS score of 3 or more, over 85% of Rocket AF patients had a CHADS score of 3 or more • RE-LY patients were about 71.5 years old, and Rocket AF patients were 73 years old • Prior stroke TIA embolism was about 20% in RE-LY and was 55% in Rocket AF • About half of RE-LY patients were warfarin naïve, whereas on 37.5% of Rocket AF patients were warfarin naive C. Michael Gibson, M.S., M.D. Rocket AF Investigators, AHA 2010; Connolly SJ, et al. N Engl J Med. 2009;361:1139-1151
Impact of Enrolling Higher CHADs Score Patients • Higher CHADs scores are associated with: • Higher rates of major bleeding • Lower TTRs C. Michael Gibson, M.S., M.D. Personal communication RE-LY Investigators. Connolly SJ, et al. N Engl J Med. 2009;361:1139-1151
Comparison of Trial Metrics C. Michael Gibson, M.S., M.D. Rocket AF Investigators, AHA 2010; Connolly SJ, et al. N Engl J Med. 2009;361:1139-1151
Rates of Drug Discontinuation RE-LY 1 Year: Dabigatran 110 mg: 14.5% Dabigatran 150 mg: 15.5% Warfarin: 10.2% 2 Years: Dabigatran 110 mg: 20.7% Dabigatran 150 mg: 21.2%, Warfarin: 16.6% Rocket AF Rivaroxaban: 23.9% Warfarin: 22.4% C. Michael Gibson, M.S., M.D. Rocket AF Investigators, AHA 2010; Connolly SJ, et al. N Engl J Med. 2009;361:1139-1151
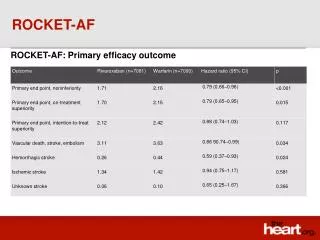
Primary Endpoint of Stroke or Systemic Embolism: Non-inferiority Analysis Non Inferiorirty p vs warfarin RE-LY Dabigatran 110 mg 1.53% per year Dabigatran 150 mg 1.11% per year Warfarin 1.69% per year Rocket AF Rivaroxaban 20mg 2.12% per year Warfarin 2.42% per year ITT Analysis p<0.001 p<0.001 Per Protocol Analysis p<0.001 No ITT analysis is available for non-inferiority in Rocket AF. An on treatment or per-protocol analysis is generally performed in the assessment of non-inferiority. If numerous patients come off of study drug, this biases the trial towards a non-inferior result in an ITT analysis. This is the basis for performing a per-protocol analysis in a non-inferiority assessment. C. Michael Gibson, M.S., M.D. Rocket AF Investigators, AHA 2010; Connolly SJ, et al. N Engl J Med. 2009;361:1139-1151
Primary Endpoint of Stroke or Systemic Embolism: Superiority Analysis Superiority p vs warfarin ITT Analysis RE-LY Dabigatran 110 mg 1.53% per year Dabigatran 150 mg 1.11% per year Warfarin 1.69% per year Rocket AF Rivaroxaban 20mg 2.12% per year Warfarin 2.42% per year p=0.34 p<0.001 p=0.117* *In an on treatment analysis in Rocket AF Stoke or SE rates were 1.70% / yr for rivaroxaban and 2.15% / yr for warfarin, p=0.015. No on treatment analysis is available from RE-LY. C. Michael Gibson, M.S., M.D. Rocket AF Investigators, AHA 2010; Connolly SJ, et al. N Engl J Med. 2009;361:1139-1151
Hemorrhagic Stroke ITT P-value HR RELY Dabigatran 110 mg 0.12% / yr 0.31 <0.001 Dabigatran 150 mg 0.10% / yr 0.26 <0.001 Warfarin 0.38% / yr Rocket AF Rivaroxaban 20 mg 0.26% / yr 0.59 0.012* Warfarin 0.44% / yr *In an on treatment analysis in Rocket AF Hemorrhagic Stoke rates were 0.26% / yr for rivaroxaban and 0.44% / yr for warfarin, p=0.024. No on treatment analysis is available from RE-LY. C. Michael Gibson, M.S., M.D. Rocket AF Investigators, AHA 2010; Connolly SJ, et al. N Engl J Med. 2009;361:1139-1151
Ischemic Stroke ITT P-value HR RELY Dabigatran 110 mg 1.34% / yr 1.20 0.35 Dabigatran 150 mg 0.92% / yr 0.76 0.03 Warfarin 1.20% / yr Rocket AF Rivaroxaban 20 mg 1.62% / yr 0.99 0.92* Warfarin 1.64% / yr *In an on treatment analysis in Rocket AF Ischemic Stoke rates were 1.34% / yr for rivaroxaban and 1.42% / yr for warfarin, p=0.58. No on treatment analysis is available from RE-LY. C. Michael Gibson, M.S., M.D. Rocket AF Investigators, AHA 2010; Connolly SJ, et al. N Engl J Med. 2009;361:1139-1151
Myocardial Infarction ITT P-value HR RELY Dabigatran 110 mg 0.72% / yr 1.35 0.07 Dabigatran 150 mg 0.74% / yr 1.38 0.048 Warfarin 0.53% / yr Rocket AF Rivaroxaban 20 mg 1.02% / yr 0.91 0.46* Warfarin 1.11% / yr *In an on treatment analysis in Rocket AF MI rates were 0.91% / yr for rivaroxaban and 1.12% / yr for warfarin, p=0.121. No on treatment analysis is available from RE-LY. C. Michael Gibson, M.S., M.D. Rocket AF Investigators, AHA 2010; Connolly SJ, et al. N Engl J Med. 2009;361:1139-1151
Major Bleeding ITT P-value RE-LY HR Dabigatran 110 mg 2.71% / yr 0.8 0.003 Dabigatran 150 mg 3.11% / yr 0.93 0.31 Warfarin 3.36 150 mg Dabigatran vs 110 mg Dabigatran = HR of 1.16 (1.00–1.34) p = 0.052 On Treatment P-value Rocket AF Rivaroxaban 20 mg 3.60% / yr 0.92 0.58* Warfarin 3.45% / yr *There is no ITT analysis of safety in Rocket AF. There is no on treatment analysis of safety from RE-LY. C. Michael Gibson, M.S., M.D. Rocket AF Investigators, AHA 2010; Connolly SJ, et al. N Engl J Med. 2009;361:1139-1151
All Cause Mortality ITT P-value HR RELY Dabigatran 110 mg 3.75% / yr 0.88 0.35 Dabigatran 150 mg 3.64% / yr 0.91 0.051 Warfarin 4.13% / yr Rocket AF Rivaroxaban 20 mg 4.52% / yr 0.92 0.152* Warfarin 4.91% / yr *In an on treatment analysis in Rocket AF mortality rates were 1.87% / yr for rivaroxaban and 2.21% / yr for warfarin, p=0.073. No on treatment analysis is available from RE-LY. C. Michael Gibson, M.S., M.D. Rocket AF Investigators, AHA 2010; Connolly SJ, et al. N Engl J Med. 2009;361:1139-1151
Conclusions: RE-LY vs Rocket AF Regarding Primary Endpoint of Stroke and/or Systemic Embolization Primary Analysis of Non-Inferiority: Both drugs were non-inferior to Warfarin in reducing the primary endpoint of stroke and systemic embolism Secondary Analysis of Superiority: In a pre-specified secondary On Treatment analysis, rivaroxaban was superior to warfarin. No On Treatment analysis is available for dabigatran versus warfarin. In an Intent-to-Treat analysis, 150 mg of dabigatran was superior to warfarin while rivaroxaban was not. C. Michael Gibson, M.S., M.D. Rocket AF Investigators, AHA 2010; Connolly SJ, et al. N Engl J Med. 2009;361:1139-1151
Conclusions: RE-LY vs Rocket AF Regarding Stroke Dabigatran 150 mg reduced the risk of hemorrhagic stroke (HR 0.26, p<0.001) as did rivaroxaban (HR 0.59, p=0.024). Both drugs were therefore safer. Dabigatran 150 mg also reduced the risk of ischemic stroke (HR=0.76, p=0.03) while rivaroxaban did not (p=0.58)(dabigatran was associated with thrombotic efficacy) C. Michael Gibson, M.S., M.D. Rocket AF Investigators, AHA 2010; Connolly SJ, et al. N Engl J Med. 2009;361:1139-1151
Conclusions: RE-LY vs Rocket AF Regarding Bleeding There was no difference in major bleeding associated with 150 mg of dabigatran therapy versus warfarin. There was statistically less major bleeding associated with 110 mg of dabigatran than warfarin. While there was numerically more major bleeding with rivaroxaban, there was less fatal bleeding with rivaroxaban compared with warfarin. Extracranial bleeding was numerically less with 110 mg of dabigatran than warfarin, but both 150 mg of dabigatran and rivaroxaban had numerically more extracranial bleeds than warfarin C. Michael Gibson, M.S., M.D. Rocket AF Investigators, AHA 2010; Connolly SJ, et al. N Engl J Med. 2009;361:1139-1151
Conclusions: RE-LY vs Rocket AF Regarding Mortality In the intent-to-treat analysis, there was a strong trend for a mortality reduction with dabigatran 150 mg (p=0.051) while there was a modest trend for a mortality reduction with rivaroxaban (4.52 / yr vs 4.91 / yr, p=0.152) C. Michael Gibson, M.S., M.D. Rocket AF Investigators, AHA 2010; Connolly SJ, et al. N Engl J Med. 2009;361:1139-1151