Download

1 / 25
250 likes | 283 Views
Explore the bespoke Health Research Classification System (HRCS) designed collaboratively by UK Clinical Research Collaboration, offering 21 Health Categories and 48 Research Activity Codes for comprehensive health and biomedical research funding analysis.

E N D
Health Research Classification System Dr. Ian Viney Medical Research Council (MRC) Director of Strategic Evaluation and Impact MRC Head Office (London, UK)
UK Clinical Research Collaboration (UKCRC) • The UK Clinical Research Collaboration (UKCRC) was established in 2004 with the aim of “ensuring a coherent approach to the funding of clinical research in the UK by developing a culture of communication and coordinated strategies between the major funders”. • More than 20 organisations participate in the UKCRC, including the Association of Medical Research Charities (AMRC) which represents 125 medical charities • The first step for the UKCRC was to fully describe the funding landscape – to identify gaps and opportunities for health research in the UK. • A bespoke Health Research Classification System (HRCS) was developed collaboratively, based on the Common Scientific Outline used by the US National Cancer Institute to allow meaningful comparisons to be made across the different funders’ research portfolios.
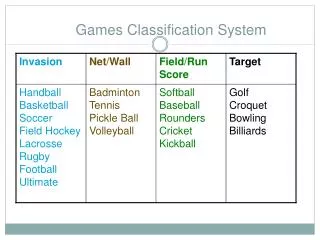
What is the HRCS? • A system for classifying and analysing health and biomedical research funding • Designed collaboratively by a range of funders • Two-dimensional system • Health Categories • Research Activity Codes • Now used internationally
Structure of the HRCS Health Categories All areas of health or disease 21 individual categories Based on WHO International Classification of Diseases Research Activity Codes All types of research activity from basic to applied 48 codes in 8 groups Based on cancer Common Scientific Outline For rules, guidelines, tutorials and other resources: www.hrcsonline.net
Musculoskeletal Neurological Oral and Gastrointestinal Renal and Urogenital Reproductive Health and Childbirth Respiratory Skin Stroke Generic Health Relevance Other Health Categories • Blood • Cancer • Cardiovascular • Congenital Disorders • Ear • Eye • Infection • Inflammatory and Immune System • Injuries and Accidents • Mental Health • Metabolic and Endocrine
Key Features of the HRCS Coding is based on the main research objective Not a keyword system Does not capture all potential downstream outcomes Complements existing coding systems Coding is linked directly to associated funding Codes based on lifetime of the award Exact percentages with every code System provides a broad overview of the centre of gravity of research An aggregate population summary Fine grained expertise not required
Advantages of the HRCS • Covers the full spectrum of all types of health and biomedical research across all areas of health and disease • Provides a single stable common system allowing meaningful comparisons across time and between different portfolios • Answers strategic questions about investment by giving a “broad brush” overview of funding patterns • Is tried and tested across a range of settings, organisations and analysis contexts
Limitations of the HRCS • Some concepts do not map onto the system • Paediatrics / Old age • As applied currently, it ignores background research and potential downstream consequences • Intended to be closely tied to funded activity • It does not capture detail • Does not replace other keyword systems or finding aids • Ignores ‘background funding’ for health research • Tied to ‘discretionary’ funds – not a financial audit • Summary totals can be misused as do not include all health research support
UK Health Research Analysis (2006) • The UK Health Research Analysis report, published in 2006 provided an overview of all types of health research activity across all areas of health and disease in the UK, funded by the largest government and charity health-related research funders.
From Donation to Innovation (2007) • From Donation to Innovation, is an in-depth analysis of research funded by medium and smaller sized members of the Association of Medical Research Charities (AMRC). This report provides a breakdown of spending by 29 charities (not included in the 2006 UK Health Research Analysis report) across all types of health research.
Impact of HRCS Analysis • Used for strategy development in many organisations in the UK • Discussion about the amount spent on prevention, respiratory medicine etc. • Interest in capacity building for translational research • Stimulated joint funding initiatives • National Prevention Research Initiative (more than £30m committed via four phases from 16 funders) • Public Health Initiative (£20m to fund 5 centres of excellence from 8 funders) • Translational Infections Research Initiative (£16.5m for new grants from 7 funders) • UK brain banking strategy (appointment of national director and greater co-ordination of activity) • Basis for discussions between UK funders on evaluation • Positive settlements for medical research in Government spending reviews • Health research funders can demonstrate positive changes as a result of improved co-ordination
2009/10 UK Analysis In 2012 a further analysis of UK health research was published, based on expenditure in 2009/10 • By utilising data from national R&D surveys, it was estimated that the total health relevant R&D spend in 2009/10 in the UK was £8.1bn • £4.4bn of this is R&D performed by the private sector • £1.6bn of direct expenditure on projects and programmes (11,500 awards vs. 9,900 in 2004/5) that could be classified by the HRCS
Health categories and burden of disease • Updated WHO data on burden of disease • Doubling of spend on prevention research (main focus on primary prevention) • Spend on respiratory medicine is 3x higher • Spend on infection research higher, despite DALYs decreasing • Spend on cancer research slightly lower as a proportion (but increased spend in real terms) • Amount spent on particular diseases depends on capacity, tractability etc.
Next Steps • ESF Science Policy Briefing launched in November 2011, followed by an implementation workshop in November 2011, a follow-up paper in May 2012 and a survey of all ESF Member Organisations with health research portfolio in summer-autumn 2012 • Use of the HRCS is encouraged as the leading approach for comparison and joint analysis of specifically health research portfolio information • We hope that publication of the 2009/10 UK analysis will help • Methodological developments are needed to reduce the cost of classification and increase flexibility • We have collaborated with Elsevier to examine approaches for automation, however improving on manual coding is difficult • Central support and funding are needed to manage and co-ordinate a common approach • We are discussing work to establish a central database for portfolio data, probably based on the federated Researchfish database for research output data (www.researchfish.com) • The UKCRC is planning a further UK-wide analysis for 2014/15 • More than 75 public and charitable research funding organisations should be involved • A review of the HRCS and updating guidance will be undertaken first
Summary • Consistent categorisation of research portfolios is essential for analysis of funding over time and across funding agencies • Funding agencies need a stable, widely implemented, and well supported categorisation system – the HRCS may be the best example of this – but unlikely to be the only solution needed • Efficient approaches for the automated categorisation of research, and methods to map classifications to the HRCS would be helpful • Maintaining this common language should be collaborative between medical research funders • Need to set the analysis in context, direct spend on projects and programmes is only part of the picture (also infrastructure, overseas contributions, private sector etc.) • Focus is shifting to the analysis of research output and the HRCS may be helpful to the categorisation of some outputs
HRCS Online website Makes all existing information and resources accessible Guidance for naïve users wanting to learn how to use the system Reference source for experienced users Provides further contextual help, summaries and linkages Overarching aim to promote sustainability of the system
Applying the HRCS • Promoting consistency and standardisation • Simple reproducible rules – equal proportions, minimum number of codes • Training sessions • Coding manual (background, guidance answers to questions etc.) • Data processing tools for collecting, checking and analysing codes • Data entry form • Database • Analysis spreadsheets • Rules and resources captured on website • www.hrcsonline.net
Live Issues (1) • Sustainability of the coding process • Who codes? Why? How? When? • How to define and ensure good practise? • How to access training and support expertise? • Evaluation of the coding process • How to check reliability within organisations? • How to monitor consistency across organisations? • Is there a place for automatic coding? (eg Elsevier)
Live Issues (2) • Wider strategic application • Coding of unfunded applications (measure demand) • Coding of completed research projects (were the objectives met?) • Coding of published studies (what were the outputs?) • International co-operation and analysis • International Cancer Research Partnership (ICRP) example (www.cancerportfolio.org) • Mutually funded coordination • Sources of expertise • International control group • Annual data updates • Public central repository
Total UK Expenditure on Health Research • 12 large charitable and public sector funders participated in the analysis • Private sector and some other significant funding for health research (for example neurodegenerative disease charities) is missing from the analysis • By utilising data from national R&D surveys we estimate that total health relevant research and development spend in 2009/10 in the UK was £8.1bn • £4.4bn of this is R&D performed by the private sector • £1.6bn of direct expenditure on projects and programmes that could be classified by the HRCS across the 12 participating organisations, is included • In addition £0.8bn of infrastructure funding (e.g. core support for large research units etc. which could not be categorised using the HRCS), and a small amount of funding overseas (e.g. research in Africa) was noted
2009/10 UK Health Research Expenditure • £8.1bn was spent on health research by UK organisations in 2009/10 • £2.4bn public funding, £1.1bn charity funding £4.4bn private sector funding and £0.2bn funding from overseas
2009/10 Analysis Headline Findings • Coded 11,500 awards, totalling £1.6bn spend in 2009/10, compared with 9,900 awards totalling £965m in 2004/05 • 50% more funding in real terms for health research in 2009/10 compared to 2004/05 • “Full economic costing” (2006) is part of this increase • Compared to 20% increase in pharmaceutical sector R&D spend, and 12% increase in UK GERD over the same period • 60% of public and charitable research analysed was categorised as “underpinning” or “aetiological” • Slight decrease in proportion of combined spend • These areas still received an additional £220m in real terms over the investment in 2004/05 • Interesting change in spend on research relevant to methodology development and measurement • Treatment development and evaluation has increased from 17% to 19% of the total spend – representing an additional £130m spent in these translational areas in real terms