Download
1 / 24
240 likes | 308 Views
Learn about blood culture collection, interpretation of results, rejection criteria, and post-processing steps to diagnose bacteremia. Understand how to prepare patients, avoid contaminants, and accurately interpret positive and negative blood culture results.

E N D
Only 5-15% of blood cultures are (+) in febrile patients. • Types of bacteremia: • Extravascular: via the lymphatic's. • Intravascular: i.e. CVC infections. • Types of bacteremia: • Transient: Disruption of mucosal surfaces (dental or surgical procedures). • Intermittent: Associated with abscesses. • Continuous: Infective endocarditis.
Bacteremia: Contaminants • Coagulase (-) Staphylococci. • Corynebacterium species. • Bacillus species. • If multiple isolated from separate sites are obtained, the organisms could be pathogenic. • Viridans Streptococci can be a contaminant.
Methods • Two blood cultures for separate venipuncture sites is adequate. • Three sets of blood. • At least 10ml/ venipuncture. • Blood culture > 5ml blood: 92% yield • Blood culture < 5 ml blood: 69% yield Note: Diagnostic yield increased by 3% for every 1 ml of blood drawn
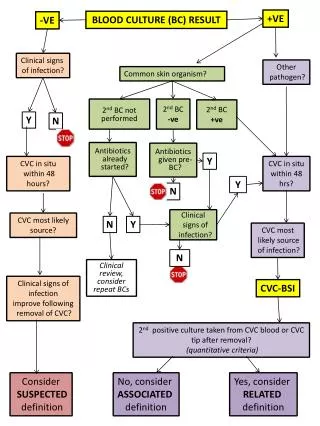
Interpretation • Organisms isolated > 72 hours are often contaminants.* • A single blood cultures with coagulase (-) staphylococci is often a contaminant.** • A single (+) blood cultures with S. Aureus, gm (-) bacillie or candida is always a pathogen and requires therapy. • The patient does not have leukocytosis or a left shift (false-positive blood cultures).
Aim of the test • Diagnosis of bacteremia by • Aerobic and anaerobic cultivation of the blood, • With identification& • Susceptibility test of the isolated organism (s). • Pediatrics: only aerobic.* • Blood culture should be made for cases with : • suspected septicemia, endocarditis, and bacteremia secondary to localized infections (pneumonia, intraabdominal abscesses, pyelonephritis, epiglottitis, meningitis).
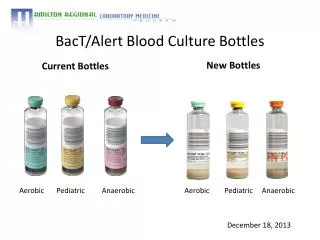
Criteria of specimen rejection • Blood collected in tubes or bottles other than aerobic and anaerobic blood culture bottles. • If the information on the label does not match that of the request form. • Specimens for anaerobic blood culture received in aerobic bottles or vice versa.
Patient preparing • The major difficulty in interpretation of blood cultures is potential contamination by skin microbiota. • So: careful attention to the details of skin preparation and antisepsis prior to collection of the specimen.
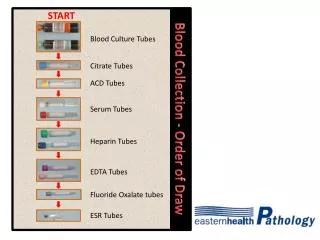
Obtaining Blood Culture • Locate the vein (usually anticubital fossa) • Attention to IV line. • Prep kit • Alcohol 5 sec. Dry 30-60 sec • Tincture of Iodine-center to periphery. Dry 45-60 sec • Remove caps, clean with alcohol • Put on gloves • Without palpating, draw 20 ml and put 10 in anaerobic and 10 in aerobic bottle. • Dispose of syringe in sharps container. • Label bottles and send to lab.
Set 1 = L. antecubital fossa at 0 minutes Set 2 = R. antecubital fossa at 30 minutes Set 3 = L. or R. antecubital fossa at 90 minutes. Best time for sample collection: during fever spike\chills. 1st sample: 90% detection.
Method • Blood is injected to both aerobic and anaerobic bottles and incubated for up to 10 days at 37 C. • Discard as negative after the 10 days • During the incubation period, a gram stain and subculture onto appropriate media should be done.
Sodium polyanethol sulphonate (SPS) • The anticoagulant in blood culture medium must not harm the bacteria and must prevent clotting of the blood, which entrap bacteria and prevent their detection . • The most commonly used preparation in blood media is 0.025% to 0.05% SPS. • In addition to it’s anticoagulant properities, SPS is also anticomplementary, antiphagocytic, and interferes with the activity of some antimicrobial agents.
Post specimen processing • Interfering factors • Patient on antibiotic therapy • Result reporting • Any isolated organism will be reported. Antibiotic sensitivity will also be included with the report. • Turn around time • Initial blood culture results will be reported as soon as it shows growth. • Final results with sensitivity will be issued after 24- 48 hours of the initial report. • Negative results will be issued after 10 days of culture submission.
Interpretation of Positive Blood Cultures • Virtually any organism, including normal microbiota, can cause bacteremia. • A negative culture result does not necessarily rule out bacteremia; • false-negative results occur when pathogens fail to grow. • A positive culture result does not necessarily indicate bacteremia; • false-positive results occur when contaminants grow.
Gram-negative bacilli, anaerobes, and fungi should be considered pathogens until proven otherwise. • The most difficult interpretation problem is to determine whether an organism that is usually considered normal skin microbiota is a true pathogen.
Limitations • Three negative sets of blood cultures in the absence of antimicrobial therapy are usually sufficient to exclude the presence of bacteremia. • One set is seldom ever sufficient. • Prior antibiotic therapy may cause negative blood cultures or delayed growth. • Blood cultures from patients suspected of having Brucella or Leptospira must be requested as special cultures, Consultation with the laboratory for special culture procedures for the recovery of these organisms prior to collecting the specimen is recommended.
Observed that performance of biphasic system to be superior in recovering Brusella spp . • The bi phasic system is feasible and practical method , it has the advantage of repeated exposure of agar medium to actively proliferating organisms in the liquid broth during sub culturing, which is simply by tilting the bottle..