Download
1 / 1
10 likes | 143 Views
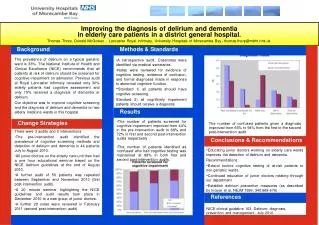
EFFECT OF A PSYCHOSOCIAL INTERVENTION ON THE SUBJECTIVE QUALITY OF LIFE, SYMPTOMATOLOGY AND SELF-CONSTRUCTION OF PEOPLE DIAGNOSED AS PARANOID SCHIZOPHRENICS Antonia Mª Gómez, Ph.D., & Luis Botella, Ph.D. FPCEE/SAAP Blanquerna Ramon Llull University Barcelona, Spain. INTRODUCTION

E N D
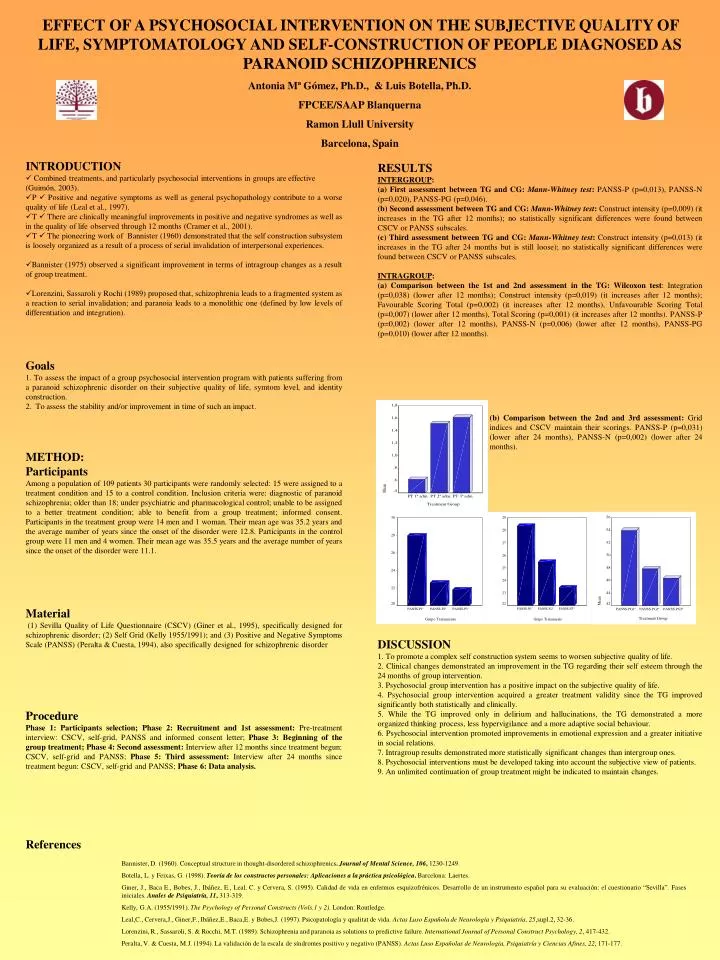
EFFECT OF A PSYCHOSOCIAL INTERVENTION ON THE SUBJECTIVE QUALITY OF LIFE, SYMPTOMATOLOGY AND SELF-CONSTRUCTION OF PEOPLE DIAGNOSED AS PARANOID SCHIZOPHRENICS Antonia Mª Gómez, Ph.D., & Luis Botella, Ph.D. FPCEE/SAAP Blanquerna Ramon Llull University Barcelona, Spain • INTRODUCTION • Combined treatments, and particularly psychosocial interventions in groups are effective (Guimón, 2003). • P Positive and negative symptoms as well as general psychopathology contribute to a worse quality of life (Leal et al., 1997). • T There are clinically meaningful improvements in positive and negative syndromes as well as in the quality of life observed through 12 months (Cramer et al., 2001). • T The pioneering work of Bannister (1960) demonstrated that the self construction subsystem is loosely organized as a result of a process of serial invalidation of interpersonal experiences. • Bannister (1975) observed a significant improvement in terms of intragroup changes as a result of group treatment. • Lorenzini, Sassaroli y Rochi (1989) proposed that, schizophrenia leads to a fragmented system as a reaction to serial invalidation; and paranoia leads to a monolithic one (defined by low levels of differentiation and integration). RESULTS INTERGROUP: (a) First assessment between TG and CG: Mann-Whitney test: PANSS-P (p=0,013), PANSS-N (p=0,020), PANSS-PG (p=0,046). (b) Second assessment between TG and CG: Mann-Whitney test: Construct intensity (p=0,009) (it increases in the TG after 12 months); no statistically significant differences were found between CSCV or PANSS subscales. (c) Third assessment between TG and CG: Mann-Whitney test: Construct intensity (p=0,013) (it increases in the TG after 24 months but is still loose); no statistically significant differences were found between CSCV or PANSS subscales. INTRAGROUP: (a) Comparison between the 1st and 2nd assessment in the TG: Wilcoxon test: Integration (p=0,038) (lower after 12 months); Construct intensity (p=0,019) (it increases after 12 months); Favourable Scoring Total (p=0,002) (it increases after 12 months), Unfavourable Scoring Total (p=0,007) (lower after 12 months), Total Scoring (p=0,001) (it increases after 12 months). PANSS-P (p=0,002) (lower after 12 months), PANSS-N (p=0,006) (lower after 12 months), PANSS-PG (p=0,010) (lower after 12 months). Goals 1. To assess the impact of a group psychosocial intervention program with patients suffering from a paranoid schizophrenic disorder on their subjective quality of life, symtom level, and identity construction. 2. To assess the stability and/or improvement in time of such an impact. (b) Comparison between the 2nd and 3rd assessment: Grid indices and CSCV maintain their scorings. PANSS-P (p=0,031) (lower after 24 months), PANSS-N (p=0,002) (lower after 24 months). METHOD: Participants Among a population of 109 patients 30 participants were randomly selected: 15 were assigned to a treatment condition and 15 to a control condition. Inclusion criteria were: diagnostic of paranoid schizophrenia; older than 18; under psychiatric and pharmacological control; unable to be assigned to a better treatment condition; able to benefit from a group treatment; informed consent. Participants in the treatment group were 14 men and 1 woman. Their mean age was 35.2 years and the average number of years since the onset of the disorder were 12.8. Participants in the control group were 11 men and 4 women. Their mean age was 35.5 years and the average number of years since the onset of the disorder were 11.1. Material (1) Sevilla Quality of Life Questionnaire (CSCV) (Giner et al., 1995), specifically designed for schizophrenic disorder; (2) Self Grid (Kelly 1955/1991); and (3) Positive and Negative Symptoms Scale (PANSS) (Peralta & Cuesta, 1994), also specifically designed for schizophrenic disorder DISCUSSION 1. To promote a complex self construction system seems to worsen subjective quality of life. 2. Clinical changes demonstrated an improvement in the TG regarding their self esteem through the 24 months of group intervention. 3. Psychosocial group intervention has a positive impact on the subjective quality of life. 4. Psychosocial group intervention acquired a greater treatment validity since the TG improved significantly both statistically and clinically. 5. While the TG improved only in delirium and hallucinations, the TG demonstrated a more organized thinking process, less hypervigilance and a more adaptive social behaviour. 6. Psychosocial intervention promoted improvements in emotional expression and a greater initiative in social relations. 7. Intragroup results demonstrated more statistically significant changes than intergroup ones. 8. Psychosocial interventions must be developed taking into account the subjective view of patients. 9. An unlimited continuation of group treatment might be indicated to maintain changes. Procedure Phase 1: Participants selection; Phase 2: Recruitment and 1st assessment: Pre-treatment interview: CSCV, self-grid, PANSS and informed consent letter; Phase 3: Beginning of the group treatment; Phase 4: Second assessment: Interview after 12 months since treatment begun: CSCV, self-grid and PANSS; Phase 5: Third assessment: Interview after 24 months since treatment begun: CSCV, self-grid and PANSS; Phase 6: Data analysis. References Bannister, D. (1960). Conceptual structure in thought-disordered schizophrenics. Journal of Mental Science, 106, 1230-1249. Botella, L. y Feixas, G. (1998).Teoría de los constructos personales: Aplicaciones a la práctica psicológica. Barcelona: Laertes. Giner, J., Baca E., Bobes, J., Ibáñez, E., Leal, C. y Cervera, S. (1995). Calidad de vida en enfermos esquizofrénicos. Desarrollo de un instrumento español para su evaluación: el cuestionario “Sevilla”. Fases iniciales.Anales de Psiquiatría, 11, 313-319. Kelly, G.A. (1955/1991). The Psychology of Personal Constructs(Vols.1 y 2). London: Routledge. Leal,C., Cervera,J., Giner,F., Ibáñez,E., Baca,E. y Bobes,J. (1997). Psicopatología y qualitat de vida. Actas Luso Española de Neurología y Psiquiatría, 25,supl.2, 32-36. Lorenzini, R., Sassaroli, S. & Rocchi, M.T. (1989). Schizophrenia and paranoia as solutions to predictive failure. International Journal of Personal Construct Psychology, 2, 417-432. Peralta, V. & Cuesta, M.J. (1994). La validación de la escala de síndromes positivo y negativo (PANSS). Actas Luso Españolas de Neurología, Psiquiatría y Ciencias Afines, 22, 171-177.