Download
1 / 20
200 likes | 335 Views
Improving referral systems for people with mental health problems in police custody. Alison Pearsall.

E N D
Improving referral systems for people with mental health problems in police custody Alison Pearsall
Aims To improve efficiency and effectiveness of clinical care/service provisionTo maximise service standards by removing barriers, bottle necks and smoothing transitionsDiagnostic for service improvements involving frontline staffTo improve individuals’ care experience
Objectives Define where the process starts and ends Identify individual activities including timescales Assemble the pathway to create the journey (parallel activities) Note the issues and opportunities
Setting the context 80% of problems with care delivery is about the system not the people 30 - 70% of work in the NHS does not add value for service users up to 50% of process steps involve handover or transition = increasing the risk of error, duplication and delay
DMAIC – MH in police custody Assessment, movement and aftercare through police custody No current measurement established, no care pathway or clinical outcomes Storage of information, making referrals and arranging aftercare Assessment process & communication Underpin with policy, procedures and agreements across services and agencies Define Measure Analyse Improve Control
parallel to the legal framework Remand CPS Bail Police Urgent assessment process Routine assessment process Ongoing treatment/support process MH in police custody Court
Themes 12 Themes: 1. Communication 2. Hand offs 3. Documentation 4. Room changes 5. Admin time 6. IT 7. Staff involved 8. Dual/repeat processes 9. Transportation 10. Contact relatives 11. Referrals 12. Outcomes
1. Complex communication and activityReferral/assessment/liaison alongside charge/interview/prosecution Cells CJL team release M H ass’ment records interview CPS Custody CID/ PPU legal advice Finger prints Medacs & Submisuse arrest
2. Hand overs/responsibilities/transitions Submisuse Screening CJL Screening Arrest/ Entry to Police Custody Legal Process Finger prints/ Case building Decision to prosecute Custody Sergeant FME/Medac MH Ass’ment Referral & f/up Exit from Custody (bail, court, remand, hospital, release)
Arrest/entry to police custody Detailing the assessment process Stages of the journey through custody Exit from Custody (bail, court, remand, hospital, release)
Analysing the Map • How many steps/variations in the process? • How many duplications? • How many hand-overs/transitions? • What is the approx. time of, or between, each transition? • Where are possible delays? • Where are major bottlenecks? • How many steps do not ‘add value’ for patient? • Where are the problems for patients and staff?
Analysis summary Steps Total number steps 35 Number of value steps 5 Value steps as 1.75% total steps Time Total time Hrs:15 Mins:47 Time of value steps: 3 Value Time as 0.45% total time • Waste • Waiting • Mistakes • Uncoordinated activity • Motion – repeat assessment • Inappropriate processing
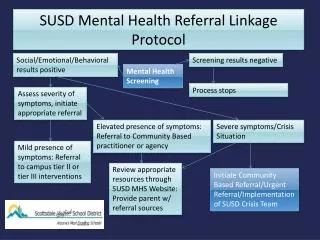
1 Police to detect MI & refer Arrest/entry to custody 3 2 Extended CJL to Police station CJL hours extended Referrals accepted Police to Identify MI & refer Screening Morning only Submisuse screen all arrestees CJS & eCPA Records check CJL staff screen all arrestees PACE timescales 6 5 Referral to PCMHT OPT in letter Referral to CMHT/CCCT 3 failed appointments SU discharged Crisis Team Gatekeeping not if too risky No follow up Paper, stamps, a stable address & be able to read SPAR to services Mental Health Assessment 4 7 Exit from custody 11. Referrals
11. REFERRALS Mental Health Assessment 5 Referral to PCMHT OPT in letter 6 7 Crisis Team Gatekeeping not if too risky No follow up Referral to CMHT/ CCCT 3 failed contacts = discharge Paper, stamps, a stable address & be able to read - SPA to services Exit from custody
Assessment and referral processes are often influenced by PACE, MH legislation and the need to co-ordinate the two processes Clinical assessment Identifying issues Clinical decisions Referral for aftercare Release from custody Local teams need to understand and assist by accepting assessments to improve flow and release from custody Improve the referral process Change in practice - ‘opt in’ and ‘three strikes’ Local teams may require interim support from CJMHT to provide transitional care for offenders leaving custody
Future Work • MDO Meetings • S.136 Policy review • Transitional Policy • Focus groups - Community Mental Health Teams • Funding Bid
Process Mapping • Effective tool • Easy to use • Front line staff – MDT • Efficient use of time • Naturally leads to future work • Complements other data
Acknowledgements Thanks to: • Supervisors: Professor Jenny Shaw Dr Dawn Edge Dr Mike Doyle • NIHR for fellowship funding • Manchester University • Lancashire Care NHS Foundation Trust • All Service users, family, NHS, police & prison staff for participation in the study
Thank you Alison Pearsall alison.pearsall@postgrad.manchester.ac.uk