Download

1 / 49
520 likes | 778 Views
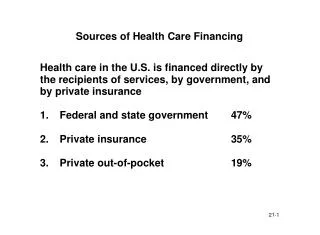
Topic: National Health Insurance in Taiwan. Group members: Jodie KWONG (04427778G) Lawrence CHAN (04703452G) Phiona SO (04726717G Remus Au (04726219G) Vicky LAM (04727185G). Agenda of Presentation. Policy directions Strategies and measures adopted Capacity building & access

E N D
Topic: National Health Insurance in Taiwan Group members: Jodie KWONG (04427778G) Lawrence CHAN (04703452G) Phiona SO (04726717G Remus Au (04726219G) Vicky LAM (04727185G)
Agenda of Presentation • Policy directions • Strategies and measures adopted • Capacity building & access • Control cost and improve efficiency • Quality assurance
Policy Directions • To further improve capacity and convenience to access • Budget containment • To further improve quality
Medical Care Network Plan • Implemented by the Department of Health (DOH) since July 1985 • 15 years, 3 Phases • Divided into 17 medical regions • 63 sub-regions
Objective of MCNP • shrink the gap of medical resources between medical regions • avoid the resources being repeatedly invested and wasted • better distribution of medical resources
3 Phases of Medical Care Network Plan Phase One and Two • 10 years (1985 - 1995) • Develop primary & secondary care - Encourage private investment in rural and mountain areas - Western and Traditional Chinese Medical mix - 100% private dental care - Free vaccinations to infant / children - Vision check up until 5 years old - Free pre-natal screening
3 Phases of Medical Care Network Plan Phase Three • 5 years (1996 - 2000) • Rehabilitation - drug rehabilitation • Long-term Care - home care service for chronic illness, day care centre, cancer care & chronic hospital etc. • Psychiatric Care - psychiatric rehabilitation centre • Quality assurance
Outcome of MCNP • the unequally distributed medical resources have been improved • By the end of 2003, over 90 percent (17,259 in total) of medical institutions in Taiwan had joined the NHI program. After the successful of MCNP, checking the efficiency of the use of medical resources has become an important task.
Competition – Internal Market • Fee-for-service • Over 16,000 healthcare providers • Improve quality of service to attract patients (focus group, patient satisfaction survey)
For improving and strengthening emergency care services in every township located in mountainous areas, outlying islands, and other areas with relatively limited medical resources, 200 health rooms / stations have been set up to serve residents in inaccessible areas. Since 1979, the government has been sending mobile medical teams to remote villages on a regular basis. In 1988, a telecommunications medical care program was initiated to provide emergency medical care for the island's residents. Removable of Geographical Barrier
Since 1995, teaching hospitals, medical centers, and regional hospitals have joined the distance medical care network and provided services to health stations in remote areas.The government also offers incentives, such as:Increased pay and commuting subsidies for medical personnel serving in rural and remote areas.Since 1975, medical school graduates who have studied on governmentscholarships are assigned to remote areas or special medical branches for six years. In 1999, an integrated delivery system was established. Removable of Geographical Barrier
“Improvement of Medicare in the Mountain and Remote Areas and Outlying Islands”(改善山離島偏遠地區醫療服務措施)By the end of 2003,48 medical service areas and 30medical institutions had joined the program, with medical service accessibility in these areas considerably improved. Removable of Geographical Barrier
The NHI benefited 400,000 people suffering from serious or terminal illnesses.The NHI cushioned the high hospitalization expenses incurred from premature babies.NHI extended coverage to the eight million citizens who were formerly uninsured, mainly the elderly, children, students, housewives, and the disabled. Removable of Financial Barrier
Removable of Financial Barrier By the end of 2004, 99 percent of the total population were covered by the NHI program.
Strategies to Control Cost and to Promote Efficiency • Macro management: Global budget • Micro management: Pharmaceutical Price List • Case payment based on DRGs • Relative Value Fee Schedule (RBRVS) Performance/Quality-based payment system: Disease/outcome Management Family physician
Macro management:Global Budget Payment Reform 1998Dental care (8.28%) 1999Traditional Chinese Medicine (4.63%) 2001Clinics (22.4%) 2002Hospitals (inpatient & outpatient) (64.69%) * ( ) percent of total cost in 2001
Macro management:Global Budget • To enhance financial responsibility of the providers and payers • To sharp providers’ cost-effective behaviors • Reallocate budget to maximize value of money Budget-driven deliver More health than health care
Macro management:Global Budget • Set expenditure cap prospectively (fixed budget floating conversion factor) thru negotiation • Allocate sector budget for different providers • Set regional budget (money follow patients)
Global Budget National Cost/health Target Regional budget Risk-adjusted capitation Capitation plan (carve-out) Peer pressure Competition Integration Sector budget Division budget • Payment reform FFS Region Payment system Case(capital • Fee Schedule • Guideline Provider Utilization Review Shapingbehavior Strategies to Control Cost and Improve Health under Global Budget
Using a set of mixed payment methods, the single payer Bureau of National Health insurance (BNHI) pays by: • Fee-for-service based on national, uniform fee schedules (RBRVS) • Diagnostic-related-groups (DRGs) for hospitals (50 DRGs as of 2002; ongoing expansion • Capitation for residents in remote mountainous areas and off-shore islands • Fee-for-performance (FFP) based on both process and outcome of care
Micro management: • Reform co-payment: 7 times(1995- 2005) ↑co-payment of outpatients ↑co-payment for prescription drugs (>$NT 100) • Drug payment price adjustment 7 times • Require referral for hospitals outpatient care or high cost (2005) • Establish Family Physician Initiatives (gate keeping, on pilot project now) and referral system (2004)
Co-payment for Ambulatory Care Bureau of National Health Insurance 2005
Micro management: RBRVS Resource Based Relative Value Scale • July 2001 • To serve as the foundation for payment system • Mainly taking reference from US concept • By fixing points for various medical services • To rationally reflect the value of resources put in • First edition completed at Mar, 2003
Micro management:Case-payment Scheme • Similar to the Diagnosis- Related Group (DRG) reimbursement system in U.S. • Classified by BNHI • Approximately 50 types of medical procedures e.g. C-section, hernia repair, kidney transplant…. • At a fixed number of points
Micro management:Quality-Based Payment • Started on October 01, 2001 • 5 major diseases- cervical cancer, breast cancer, diabetes, tuberculosis, and asthma. • Provides extra financial rewards to providers in addition to the NHI fee schedule. • Finance of these extra rewards is not from global budgets. • 2003, include more diseases to the project (namely cancer, hypertension, chronic B and C-type hepatitis…)
Efficiency Enhancement • Use of IT systems • Contracting with healthcare providers • Competition among healthcare providers
Use of IC Card – Increase Clinical efficiency NHI IC card Explicit Data IC Chip Basic Data Section Healthcare Data Section Medical Data Section Health Administration Data Section Name ID Number Birth date Photograph (Optional)
Other IT Support – Increase Operating Efficiency • Use of Internet • Voice service systems
Knowledge Management • E-health learning to improve the uneven medical resources:- 1. Telemedicine 2. E-journals 3. Video-conferencing 4. Video-on-demand
Quality Assurance Accreditation of hospital • Taiwan Joint Commission on Hospital Accreditation in 1999 (TJCHA) • Integrated quality system for the entire Taiwan health care system • Taiwan Quality indicator Project in 1999 (TQIP) • Health Quality Improvement Circle in 2002 (HQIC)
Quality Assurance • NHI subsidies in accordance with level of accreditation • Higher accreditation type receive more subsidies • Public believes higher accreditation implies better medical service • 1st in Asia to conduct hospital accreditation • Accreditation lasts for a period of 3 years • 497 hospital in 2005 • 500 hospital in 2006
Quality Assurance • Some quality indicators
Quality Assurance Accreditation of Medical School • Ensure doctors are trained to provide an adequate level of care for patients • Assure the quality of education • Independent Taiwan Medical Accreditation Council (TMAC) was established in 1999 • Accreditation criteria
Quality Assurance Accreditation Criteria • Administration of the school • The teaching • Utilization of teaching resources • On-site evaluation
Clinical Practice Guidelines (CPG) • Systematically developed statements which assist in decision making about appropriate healthcare for specific clinical conditions • CPG are tools • CPG help to evaluate & assimilate the ever-increasing amount of evidence & opinion on preferred practices, taking into consideration of local system factors • CPG do not replace clinical judgement
Perceived Benefits of CPG • Align clinical practice to scientific evidence & the local healthcare setting • Alert doctors to unwarranted practices • Optimise delivery of care in a given healthcare setting. • Reveal direction for further study • Help in designing rational approaches to uncommon problems • Facilitate clinical audit
Limitations of CPG • Skill and resources demanding • More CPG are being produced than implemented • CPG cannot be appropriate for all clinical situation & cannot address concern of all patients • Inadequate attention to the limit of evidence & system barrier can lead to faulty/inapplicable recommendation • Validity declines over time due to evolving evidence • Inattention to methodology reduces acceptance & applicability
Acknowledgement Cheng, T. M. Taiwan’s new national health insurance program: genesis and experience so far, 22(3), Health Affairs. The Policy Journal of the Health Sphere. Liu, S. L. (2005). Evaluating the efficiency of the use of medical resources in Taiwan’s medical care network: An application of data envelopment analysis, Institute of Health Care Management.The Republic of China Yearbook – Taiwan 2002(http://www.gio.gov.tw/taiwan-website/5-gp/yearbook/2002/)The Republic of China Yearbook – Taiwan 2003(http://www.gio.gov.tw/taiwan-website/5-gp/yearbook/2003/)The Republic of China Yearbook – Taiwan 2004(http://www.gio.gov.tw/taiwan-website/5-gp/yearbook/2004/)The Republic of China Yearbook – Taiwan 2005(http://www.gio.gov.tw/taiwan-website/5-gp/yearbook/)