Download
1 / 28
290 likes | 500 Views
Disruptive Behavior Overview of the NC Physicians Health Program. Michele Denker M.D N.C. Physicians Health Program www.ncphp.org. NC Physicians Health Program since 1988. Warren Pendergast MD, Medical Director Joe Jordan PhD, Clinical Director Physicians Physician assistants

E N D
Disruptive Behavior Overview of the NC Physicians Health Program Michele Denker M.D N.C. Physicians Health Program www.ncphp.org
NC Physicians Health Program since 1988 • Warren Pendergast MD, Medical Director • Joe Jordan PhD, Clinical Director • Physicians • Physician assistants • Perfusionists • Anesthesia assistants • Veterinarians, Vet Techs • Self referrals or referrals from NCMB, Colleagues, Hospitals, Residency, Family • Confidential, Records protected by NC Peer Review
Advocacy Assessment NCPHP Services Referral Education Case Management Support
NCPHP Assessments Chemical Dependency and Dual Diagnosis 59% Major Psychiatric Illnesses ( Axis1) 12% Behavioral ( Axis 11) 12% Professional Misconduct 5%
Participant Diagnoses • Alcohol/substance abuse or dependence • Axis I Major Psychiatric illnesses • Axis II Personality Disorders • Axis III (General Medical Conditions) • Neuropsychiatric (cognitive) deficits
Mood Disorders • Major Depression • Dysthymia • Bipolar Disorder • Mania, Hypomania • Mood Disorders due to… Medical condition • Substance Induced
Personality Disorders & Traits Schizoid Borderline Paranoid Antisocial Narcissistic Obsessive/Compulsive
“Physician Stereotypes” • Perfectionism • Like to be ‘In-control’ • Dedication to patients above all • Problem solvers, solution focused • Successful in achieving goals • Resist change
Co-workers Colleagues Patients Behavior Distressed Physician Trauma Family Hospital system
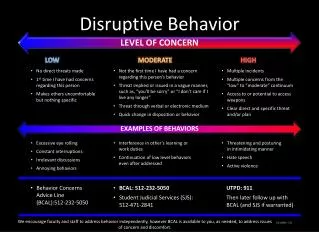
Disruptive Behavior: Definition “A physician with disruptive behavior is one who cannot, or will not, function well with others to the extent that his or her behavior, by words or actions, interferes or has the potential to interfere with quality health care delivery.” Ontario Task Force Definition
Individual Dynamics Good to excellent technicians Some OCD & Narcissism necessary Poor communication skills Poor insight into effect on others Splitting behaviors
Disruptive - Individual dynamics Control in the extreme Externalizes responsibility “He started it…” “He’s worse than I am!” Paranoia Poor boundaries
Examples of Disruptive Behavior Inappropriate Words: • Profane, disrespectful, insulting, demeaning, abusive language • Bullying , rudeness • Inappropriate arguments with patients, family members, staff • Insensitive jokes, non-clinical comments • Boundary Violations • Outbursts of anger • Negative comments about other providers
Examples of Disruptive Behavior Inappropriate actions: • Throwing or breaking things • Refusal to comply with known and generally accepted practices • Use or threat of physical force with patients, families, staff • Failure to respond to calls or persistent lateness in responding • Repeated and unjustified complaints about a colleague • Not working collaboratively with others • Rigid and inflexible requests for assistance
What Disruptive Behavior Isn’t: • Healthy criticism offered in good faith with the intention of improving patient care or facilities • Making a complaint to an outside agency • Testifying against a colleague • Good faith patient advocacy
Disruptive Behavior: Differential Diagnosis • Substance abuse • Fatigue • Stress (multiple/chronic) • Depression • Bipolar Disorder (Type I or II) • Personality Disorders • Thought disorders • Neurologic/Metabolic (delirium) • Dementia
What Works Identify early warning signs Investigate and confront disruptive behavior quickly Have system in place for problem resolution Utilize team approach to minimize splitting
Management: Documentation Verbal and written Time and place of occurrence Factual description of the behavior List of others who observed the incident(s) Consequences to patient care & staff
Management: Intervention Initial meeting: 2+ senior medical staff and administration Identify specific behaviors Explain the seriousness of the situation and the consequences of failure to change Offer help, including referral to state PHP Follow up with written summary
Management: Principles Be prepared to follow through Clear written communication Due process Equal application of bylaws Countertransference issues
Management: Principles Expectation management management vs. cure incremental change & expected backsliding Use of NCPHP Assessment is critical Differentiate treatment vs. consequences
NCPHP role NCPHP is not the Medical Board Intervention assistance Assessment Case management monitoring and feedback Support COS/medical staff Participant physician or PA
Modes of Treatment/Intervention • “Anger Management classes” • Behavioral Therapy • Coaching • Psychotherapy • Consequences in parallel
Prognosis Depends on Diagnosis/Treatment Depends on ability to gain insight Depends on ability to take responsibility Depends partly on system dynamics i.e. consistency of consequences Set goals appropriately Long-term perspective
Disruptive Behavior: Code of Conduct JCAHO Effective 1/1/09: Hospitals will have to have a code of conduct which defines acceptable and disruptive and inappropriate behaviors.
Policies & Bylaws • Clear policy & bylaws defining unacceptable behaviors • Define sanctions • Step wise process • Follow due process
Healthy professional community • Respect for colleagues and co-workers • Accept differences in others • Mentorship • Participate in team building, medical politics • Offer help and support to others • Develop willingness to reach out to others
Additional Resources http://www.cpso.on.ca/uploadedFiles/downloads/cpsodocuments/policies/positions/CPSO%20DPBI%20Guidebook%281%29.pdf