Download
1 / 32
460 likes | 1.1k Views
Ankle Sprain. A&E REHABILITATION DEPARTMENT. Ankle Sprain. Dr David Tran A&E department FVHospital Medical meeting 25/07/12. Anatomy of the external ligament. Anterior talo-fibular ligament (ATFL) Medium ligament (calcaneo-fibular = CFL) Posterior talo-fibular ligament (PTFL).

E N D
Ankle Sprain A&E REHABILITATION DEPARTMENT
Ankle Sprain Dr David Tran A&E department FVHospital Medical meeting 25/07/12
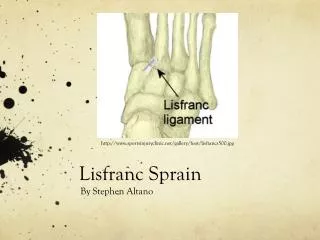
Anatomy of the external ligament • Anterior talo-fibular ligament (ATFL) • Medium ligament (calcaneo-fibular = CFL) • Posterior talo-fibular ligament (PTFL)
Ankle Sprain mechanism • Varus of the ankle (internal rotation)+/- Inversion • Often during sport activity (football, tennis, basket, jogging), sometime just walking…
Physical examination • External side of the ankle swollen • Pain at palpation of the malleola • Sometime pain at the base of the 5th metatarsus
Indication for Xray(Ottawa rules) • Patient unable to walk 4 steps • Patient more than 55 years old • Pain at one of the zones detailed here-under
Ankle laxity after ankle sprain • Xray: Dynamic view of the ankle • Laxity > 12 degree = Severe Sprain • Laxity < 12 degree = Medium Sprain
Interest of ultrasound of ligaments • The development of high-frequency transducers allows excellent visualization of ligaments. Normal ligaments are hyperechoic and are 2 to 3 mm in width. • Tear ligament is characterized by swelling of the ligament, discontinuity, redundancy, and retraction. • Ultrasound evaluation of bone is rarely requested, but the radiologist should be aware of incidental findings in bone, particularly fracture.
Ultrasound of the ankle ligament • Normal deltoid ligament. Note the navicular, talar, and calcaneal components. • Positioning of the transducer for the anterior tibiotalar portion of the ligament. • Normal anterior tibiotalar deltoid ligament (arrows). Note the triangular echogenic appearance of the ligament. • Normal tibiocalcaneal portion of the deltoid ligament. Note the hyperechoic tibiocalcaneal ligament running from the medial malleolus to the sustentaculum tali (arrows). Note also the small effusion in the ankle (arrowhead). MM, medial malleolus; SST, sustentaculum tali.
Indication of MRI ? • MRI could be indicated in case of doubt about the level of seriousness and in case of unexpected delay in the recovery period • MRI could also be indicated for professional sport competitor who need accurate diagnosis.
3 levels of seriousness • Benign sprain • Mild sprain • Severe sprain
PRICE protocol • Protection protect and stabilize the ankle joint. • Rest: stop activity to reduce the bleeding and swelling • Ice: Straight after injury, use ice twenty minutes from 3 to 6 times per day during the first three days or until swelling has substantially decreased • Compression:Wrap the injured to keep it reducing bleeding and decreasing swelling. • Elevation: Elevate the ankle higher than the heart for maximum benefit. Elevation decreases blood flow into already damaged and bleeding tissues
Treatment of benign ankle sprain • PRICE • Strapping/aircast • Duration 7-10 days • Can walk (Stop sport activity) • Rehabilitation only recommended if athlete or repetitive ankle sprain
Treatment of mild sprain • PRICE • Splint like Aircast • Duration: 21 days • Crutches 7 days • Proprioceptive rehabilitation recommended after 2 weeks
Treatment of severe sprain • PRICE • Splint or cast 45 days • Crutches • Proprioceptive rehabilitation recommended based on immobilization condition Anticoagulation with Heparin (Lovenox 40mg) daily is necessary if immobilization by Cast
ANKLE SPRAIN P.R.I.C.E. P.R.I.C.E. RE-EVALUATION J3 to 5 Benign Sprain Medium Sprain Severe Sprain
Other medical treatment • Painkillers (Efferalgan + Codeine or Tramadol) • Non Steroid Anti-inflammatory (Voltaren, Ibuprofen) • Rest and limit displacement (with crutches)
Sprain ankle with complications • Fracture of the lateral malleole (fibula) • Rupture of inter-osseous ligament • Fracture of the base of the 5th metatarsus
Do not miss other diagnosis • Fractures & Dislocation (laxity)
Other diagnosis to look for • Fracture of the base of the 5th metatarsus
ANKLE SPRAIN REHABILITATION C.COUSIN FV Hospital -Physiotherapy & Rehabilitation Department
Rehabilitation for which level of sprain? Benign Sprain Stage I Medium Sprain Stage II Severe Sprain Stage III No Rehabilitation except for: - Athlete - Ankle sprain recurrence Rehabilitation recommended Rehabilitation recommended
Ankle Sprain Rehabilitation When can you refer? • At Protective stage • For P.R.I.C.E management • For gait training with crutches • At Early Recovery stage with bracing • To re-start muscular & skeletal function • At Rehabilitative Stage • To help return back to daily and sportive activity • CAUTION: • Appropriate rehabilitation referral prevents: • Repetitive ankle sprain, later on any joints dysfunction such as knee or spine.
Techniques Ice compressive therapy Gait training with crutches PRICE PROTECTIVE STAGE Goals: 1. Decrease pain, swelling 2. Protect from over mobilization 3. Maintain appropriate weight bearing status
EARLY RECOVERY STAGEBracing is removed during rehabilitation • Goals • Decrease pain as swelling • Begin isometric strengthening • Non-weight bearing proprioceptive rehabilitation Techniques • Ice or Ice- compressive therapy • Ultrasound • Isometric exercise - neuro muscular electro stimulation • Joint alignment • Proprioception • Weight bearing pain/swelling adapted
REHABILITATIVE STAGE Goals • Increase ROM free of pain • Progress strengthening • Progress proprioceptive training • Increase pain free of activity daily living • Pain free full weight bearing • Uncompensated gait • Plyometrics exercises, agility drills, running progression
REHABILITATIVE STAGE Techniques
Rehabilitation Intervention is based on • Sprain level • Patient’s condition, • Patient’s goals, 3 to 12 rehabilitation’s sessions could be recommended
! Recurrent ankle sprain At all stages, rehabilitation is recommended for: • Joint alignment • Intensive proprioceptive program