Download
1 / 74
750 likes | 1.02k Views
SGD: SPINE A Cautionary Tale. BLOCK 5. GENERAL DATA. ALANGILAN, Ronalyn 21/F Nursing Student Right-handed Sta. Ana Manila DOA: October 1, 2009. HISTORY of PRESENT ILLNESS. 2 months PTA (+) nape pain, VAS 4-5/10 (+) fatigue ; (+) easy fatigability (-) sensory deficits

E N D
SGD: SPINEA Cautionary Tale BLOCK 5
GENERAL DATA ALANGILAN, Ronalyn 21/F Nursing Student Right-handed Sta. Ana Manila DOA: October 1, 2009
HISTORY of PRESENT ILLNESS 2 months PTA (+) nape pain, VAS 4-5/10 (+) fatigue; (+) easy fatigability (-) sensory deficits (-) bowel and bladder incontinence (+) Consult with private MD unrecalled meds, no relief
HISTORY of PRESENT ILLNESS 2 weeks PTA (+) bilateral LE weakness, left first then right (+) difficulty in ambulation - community ambulator (-) sensory deficits (-) bowel and bladder incontinence (+) Consult with albularyo no relief
HISTORY of PRESENT ILLNESS 1 week PTA (+) bilateral LE numbness (+) constipation (+) urinary retention (+) difficulty in ambulation - home ambulator with help
HISTORY of PRESENT ILLNESS 1 day PTA (+) consult at PGH ED foley catheter inserted; for OPD ff-up
HISTORY of PRESENT ILLNESS On day of admission (+) consult at PGH ED; laboratories and imaging done admitted at spine unit-Pay. ROS: (-) weight loss, (-) cough and colds, (+) intermittent fever lysed with paracetamol, (+) slight DOB; (+) malaise, (+) easy fatigability, (+) dysuria, (+) urinary retention, (-) night sweats (+) constipation, (-) Hx of trauma
PAST MEDICAL HISTORY (+) PTB exposure – school No previous hospitalizations No food or drug allergies
FAMILY MEDICAL HISTORY (-) PTB (+) HTN – father (-) DM, BA, CA, goiter, liver disease, kidney disease, heart disease
PERSONAL SOCIAL PROFILE No vices 2nd year nursing student with ward and local health center exposure 1 non-promiscuous sexual partner Lives at home with mother and sibling in a 2-storey building; father works abroad as a seaman
PE on ADMISSION Stretcher-borne, awake, coherent, NICRD BP 110/70 HR 76 RR20 Tempafebrile AS, PC, (-) CLAD, (-) NVE, (-) ANM ECE, CBS, (-) r/w AP, DHS, NRRR, (-) murmur Soft, flabby, nontender abdomen, NABS PNB, FEP, GCR, (-) cyanosis, (-) edema GCS 15, oriented to 3 spheres, CNs intact
NE on ADMISSION UPPER LIMB MOTOR FUNCTION R L C55 5Elbow flexors C65 5Wrist extensors C75 5Elbow extensors C85 5Finger flexors T15 5Finger abductors
NE on ADMISSION LOWER LIMB MOTOR FUNCTION R L L20 0Hip flexors L30 0Knee extensors L40 0Ankle dorsiflexors L50 0Long toe extensors S10 0Ankle plantar flexors S4-S5 (-) bowel incontinence
NE on ADMISSION SENSORY FUNCTION: Light Touch R L C2-T52 2 T6-L2 1 1 L30 1 L40 0 S4-S50 0
NE on ADMISSION SENSORY FUNCTION: Vibration (+) vibration, UE (+) decreased, R ASIS (-) L ASIS (-) bilateral patella
NE on ADMISSION REFLEXES R L Biceps2+ 2+ Triceps 2+ 2+ Brachioradialis2+ 2+ Patellar 3+ 4+ (+) babinski, B Ankle 4+ 4+ (+) clonus, B
LABS on ADMISSION CBC:Hgb114, Hct 0.349, WBC 8.8, Plt Ct 287, Neut% 0.890, Lymph 0.101%, Mono% 0.007, Eos% 0.000, Baso% 0.002 AFB SMEAR x 3: No acid fast bacilli seen URINALYSIS: yellow, turbid, SG 1.030, pH 6.5, RBC 3/hpf↑, WBC 7/hpf↑, Bacteria 8,536/hpf↑, few epithelial cells, no casts
LABS on ADMISSION PT:13 / 12.9 / 0.91 / INR 1.24 aPTT: 36.9 / 33.1 ECG: Sinus rhythm, normal axis BLOOD CHEM: BUN 3.53, Crea43, Na 141, K 3.9 URINE GS/CS:100,000 colonies of E. coli
T1 T2 T3 T4
SUMMARY OF THE CASE • 21/F Nursing Student with a chief complaint of neck painand history of PTB exposure • 2-week history of progressive sensory deficit with deficit starting T6 level • 1-week history of progressive motor deficit with deficit starting L2 level • Associated with fever, malaise, easy fatigability, & urinary and bowel changes; (-) weight loss, (-) anorexia • Normal pulmonary PE w/ (-) AFB smear; (-) cough • UMN signs:hyperreflexia with babinski and clonus • MRI showing compressive deformity of vertebra of T1-T2 level with soft tissue involvement
ASSESSMENT Spinal Cord Compression, ASIA B, C7 last normal level, compression deformity T1-T2 level secondary to Pott’s disease
POTT DISEASE “…a tuberculousosteomyelitis of the spine that leads to compression of vertebral bodies and a highly characteristic kyphotic deformity at the thoracic or upper lumbar level ”
POTT PARAPLEGIA “…pus or caseous granulation tissue may extrude from an infected vertebra and gives rise to an epidural compression of the cord ”
PATHOPHYSIOLOGY • Result of activation of tuberculosis at a site established by hematogenous spread. • Infectious endarteritis causes bone necrosis and collapse of a thoracic or upper lumbar (less often cervical) vertebral body resulting in a highly characteristic angulated kyphotic deformity.
CLINICAL PRESENTATION • Slight compression/mild symptoms • pain in the back • slight muscle weakness • Tingling sensation • other changes in sensation • difficulty initiating and maintaining an erection (erectile dysfunction, in men) • Pain may radiate down a leg, sometimes to the foot • exaggerated reflexes • muscle spasms and increased sweating
CLINICAL PRESENTATION • Substantial compression/severe symptoms • block most nerve impulses • severe muscle weakness, numbness • paralysis and complete loss of sensation • loss of bladder and bowel control • A belt-like band of discomfort may be felt at the level of spinal cord compression. • Once compression begins to cause symptoms, damage usually worsens from minimal to substantial unpredictably but rapidly in a few hours to a few days.
American Spinal Injury Association (ASIA) Classification • A - "complete" spinal cord injury • no motor or sensory function is preserved in the sacral segments S4-S5. • B - "incomplete" spinal cord injury • sensory but not motor function is preserved below the neurological level and includes the sacral segments S4-S5. • C - "incomplete" spinal cord injury • motor function is preserved below the neurological level and more than half of key muscles below the neurological level have a muscle grade of less than 3, which indicates active movement with full range of motion against gravity.
D - "incomplete" spinal cord injury • motor function is preserved below the neurological level and at least half of the key muscles below the neurological level have a muscle grade of 3 or more. • E - "normal" • it is possible to have spinal cord injury and neurological deficits with completely normal motor and sensory scores.
Clinical Syndromes associated with incomplete spinal cord injuries • Central cord syndrome • associated with greater loss of upper limb function compared to lower limbs • Brown-Séquard syndrome • injury to one side with the spinal cord, causing weakness and loss of proprioception on the side of the injury and loss of pain and thermal sensation of the other side • Anterior cord syndrome • injury to the anterior part of the spinal cord, causing weakness and loss of pain and thermal sensations below the injury site but preservation of proprioception that is usually carried in the posterior part of the spinal cord.
Tabes Dorsalis • injury to the posterior part of the spinal cord, usually from infection diseases such as syphilis, causing loss of touch and proprioceptive sensation. • Conus medullaris syndrome • injury to the tip of the spinal cord, located at L1 vertebra. • Cauda equina syndrome • injury to the spinal roots below the L1 vertebra.
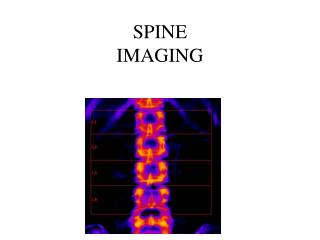
Radiologic Findings • Lytic destruction of anterior portion of vertebral body • Increased anterior wedging • Collapse of vertebral body • Reactive sclerosis on a progressive lytic process • Enlarged psoas shadow with or without calcification • Intervertebral disk spaces are decreased or obliterated • Fusiformparavertebral shadows suggest abscess formation
Day 0 – narrowed intervertebral disk space, hazy vertebral body edges Day 14 – collapse of vertebral bodies
MRI Bilateral psoas abscesses are frequent complication in lumbar involvement
Axial T2 demonstrate marrow edema at L2-L4. Right paraspinal rim enhancing fluid is demonstrated compatible with a paraspinal abscess.
DIAGNOSIS • The diagnosis still depends on biopsy for culture and pathologic examination of the affected tissue because radiographs are not diagnostic. • Imaging modalities such as CT or MRI however help target the biopsy site. • It is mentioned that MRI is the modality of choice because it can discriminate between abscess and granulation tissue and can delineate soft tissue masses and identify the amount of bone destruction.