Download
1 / 92
980 likes | 1.37k Views
Cervical Spine and Spinal Cord Injuries. Spinal Cord Injury : Epidemiology. 12 to 53 per million population per year in the U.S.A. 12,000 new paraplegics & quadriplegics per year 4000 deaths per year in the field 1000 deaths per year in hospital

E N D
Cervical Spine and Spinal Cord Injuries
Spinal Cord Injury : Epidemiology • 12 to 53 per million population per year in the U.S.A. • 12,000 new paraplegics & quadriplegics per year • 4000 deaths per year in the field • 1000 deaths per year in hospital • Lifetime care costs now > $1,000,000 per case
Spinal Cord Injury (SCI) : Etiology • Motor vehicle crashes : 46 % • Falls : 26 % • Diving / Sports : 11 % • Gunshot wounds / stabbings : 10 %* • Miscellaneous : 7 % * > 50% of SCI in some cities such as Detroit are due to gunshot wounds (GSW's)
Indications to Get Cervical Spine Films for Trauma • Appropriate mechanism of trauma • Neck pain • Neck tenderness (palpate under cervical collar) • Decreased pain perception • Head trauma (sufficient to affect mental status) • Alcohol or drugs • Children < 2 years old • Mentally retarded or dementia • Penetrating trauma • Neurologic symptoms or findings • ? if another painful distracting injury
Cervical Spine Radiology Film Choices • 3 view : cross-table lateral + odontoid + AP • 5 view : 3 view + right & left obliques • 3 or 5 view + flexion / extension • Swimmer's view to see lower C-spine • Computed tomography (CT) • Conventional tomography • Magnetic Resonance Imaging (MRI) Note : No advantage shown for 5 view over the 3 view series
MRI scan showing prevertebral edema (white arrows), cord injury (open arrow), and bone marrow edema
MRI scan showing spinal cord hemorrhage and rupture of the posterior longitudinal ligament
The Myth of the "Occult" Cervical Spine Fracture • Reviewed by Holliman & Wuerz : Amer. Journal Emer. Med., Nov. 1992 ; 10 (6) : 611-612. • All previous reported "occult" cases (with 2 poorly documented exceptions) had intracranial injury, intoxication, neck pain or tenderness, and / or neurologic signs • Two large prospective series (see next 2 slides) showed no fractures in patients not having one of the features listed on the previous slide under "indications for C-spine films" • This also was validated by the report of the NEXUS study in the year 2000
1992 Los Angeles Prospective Study on Cervical Spine Trauma Films • Hoffman et al., Ann Emer Med 1992 ; 21 : 1454-1460. • 974 cases from 1987 to 1989 • 27 C-spine fractures identified • All had midline tenderness or decreased alertness, except : • One with no pain or tenderness but blood alcohol > 200 mg % • One with distracting pelvic & femur fractures (? poor documentation of symptoms by the housestaff for this case)
1996 Los Angeles Prospective Study of Asymptomatic Trauma Patients • Velmahos et al., J Trauma 1996 ; 40 : 768-774. • 549 cases from July 1994 to June 1995 • Inclusion criteria : • Collared, alert, cooperative, no alcohol on breath • No cervical pain or tenderness, or pain on motion (3 steps) • Results : "no acute cervical spine pathology" in any of these patients • Potential cost savings by not X-raying these patients : $ 242,000
The National Emergency X-Radiography Utilization Study (NEXUS) • Started in 1998 • 21 participating medical centers • Reported in NEJM (Hoffman et al., 343 : 94-99) in July 2000 on 34,069 enrolled patients • 818 cases had cervical spine injury • The 5 "low risk" criteria identified all but 2 clinically significant C-spine injuries (negative predictive value 99.8 %) • The "low risk" criteria if applied would have avoided radiographic imaging in 12.6 % of the patients
The Five "Low Risk" Criteria Identified by the NEXUS Study • No midline cervical tenderness • No focal neurologic deficit • Normal alertness • No intoxication • No painful other distracting injury Most emergency physicians now think that if the patient does not have any of these 5, then cervical radiographs are not needed (note the additional considerations on the earlier slide)
Cervical Trauma : Indications for Computed Tomography • Lower cervical spine not seen well on lateral (must be able to see all 7 vertebrae and the top surface of T1 for lateral plain film to be regarded as adequate) • Vertebral body burst fractures • Suspected posterior column fractures • A suspected, but not clearly defined, fracture on plain films • Marked osteoarthritis present
Cervical Trauma : Indications for Conventional Tomography • Suspected fracture at base of odontoid (if only conventional CT available ; spiral CT visualizes odontoid fractures well) • Computed tomography (CT) scan marred by streak artifact from metal • Suspected facet fractures • Patient is too heavy (> 350 lbs. or 160 kg.) for the CT scanner
Cervical Trauma : Indications for Flexion / Extension Views* • Mild subluxation but no fracture seen • Prevertebral soft tissue swelling but no fracture seen • Spinal cord injury with normal plain films & CT scan • Persistent severe neck pain with normal screening films. If done, the flexion & extension should always be directly supervised by a physician, and stopped at the point at which the patient develops any increased pain or neuro symptom. * Note : These can also be considered indications for (if available) stat Magnetic Resonance Imaging (MRI) scan.
Cervical Spine Injury : Clinical Assessment • ABC's first (include "hard" immobilization) • Maintain immobilization, but open the collar & palpate neck & observe anterior neck • Clinical assessment features: • Pain / tenderness • Deformity / step-off • Edema / ecchymosis • Muscle spasm • Head position / abnormal tilt • Tracheal deviation / hematoma
Spine Injury : Neurologic Assessment • Motor strength • Sensory disturbances • Reflex changes • Autonomic dysfunction • Rectal sphincter tone
Clinical Findings : Cervical Cord Injury • Flaccid arreflexia • Diaphragmatic breathing • Pain response above clavicle only • Motor response limited to forearm flexion • Priapism • Neurogenic shock
Specific Spinal Cord Injury Syndromes • Brown-Sequard Syndrome : • Lateral hemisection of the cord • Ipsilateral motor paralysis & contralateral loss of pain & temperature sensation • Central Cord Syndrome : • Motor & sensory dysfunction worse in the upper than the lower extremities • Anterior Cord Syndrome : • Motor paralysis & loss of pain & temperature sensation ; vibration & position sense preserved • Posterior Cord Syndrome : loss of position & vibration sense only
Neurogenic Shock from Spinal Cord Injury • Due to loss of sympathetic outflow • Basically is peripheral vasodilatation & venous blood pooling • Hypotension usually also with bradycardia • Rx with IV fluids +/- alpha agonists (norepi or dopamine drip, ephedrine) +/- atropine • IV methylprednisolone 30 mg/kg (indicated if < 8 hours from time of injury)
Cervical Spine Injury : "Spinal Shock" • Is an "electrical" or depolarization injury • NOT a circulatory phenomenon • May represent electrical "stunning" of cord function • Occurs immediately after time of injury • Features: • Flaccidity • Loss of reflexes • Can have full recovery in some patients
Treatment of Cervical Fractures and Suspected Spinal Cord Injury • Maintain immobilization in hard collar • Avoid traction / distraction • Film rest of spine (T-spine & L-spine) if any sensory deficit present • Support circulation with IV fluids +/- alpha vasopressors if neurogenic shock • Antibiotics if open fracture • Neurosurg. / ortho. consult (consider transfer) • High dose steroids if SCI
Effectiveness of High Dose Steroid Rx of Spinal Cord Injuries • The Second National Acute Spinal Cord Injury Study (NASCIS II) • Results reported in New Eng. J. Med. 1990 ; 322 : 1405-1411 • Prospective, randomized, double-blind, placebo control multicenter study • Compared high dose methylprednisolone vs. naloxone vs. placebo • Found that naloxone was not effective
Conclusions of NASCIS II Study • Methylprednisolone (Solu-Medrol) at a dose of 30 mg/kg bolus followed by IV drip at 5.4 mg/kg/hr for 23 hours : • Significantly enhances recovery (both motor & sensory) from complete & incomplete acute spinal cord injuries, IF started within 8 hours of injury However, many emergency physicians now think that the benefits of the steroids are very limited (improvement of only one or 2 spinal levels in the paraplegic patient) and there are increased complications (infections, peptic ulcers / GI bleeding) from the steroids
Results of the Third National Acute Spinal Cord Injury Trial (NASCIS 3) • Better motor recovery if methylprednisolone (MP) 5.4 mg/kg/hr IV drip continued for 48 hours in patients first treated with bolus MP 3 to 8 hours post-injury • Recovery rates were the same for using MP drip for just 24 hours (if Rx started < 3 hours from injury) as for using tirilazad (a potent lipid peroxidation inhibitor) 2.5 mg/kg bolus IV q 6 hours for 48 hours • Complications were less in the tirilazad group
Indications for Emergent Surgery for Cervical Spine Injuries • Acute anterior cord syndrome • Ascending level of neuro deficit • Compound (open) fracture • GSW's • Other penetrating trauma • Associated posterior pharyngeal trauma • Pedicle fracture with nerve root symptoms • Vertebral artery injury • Note that any wound that penetrates the platysma should be evaluated by a surgeon , & usually surgically explored (may need preop esophagoscopy or gastrografin swallow and / or angiography to R/O esophageal or vascular injury)
C-Spine Trauma : What to Look for on Lateral Films • All 7 vertebrae and top of TI • 3 lines : • Anterior edge of vertebral bodies • Posterior edge of vertebral bodies • Anterior edge of spinous processes • Prevertebral space • C2 to C4 : < 5 mm ; below C4 : < 22 mm • Predental space • Adults : < 3mm ; Children : < 5 mm • Bony structures, facet joints • Soft tissues • Skull and mandible These two lines define the spinal canal
What to Look for on the A-P Radiograph • Interspinous distance > 1.5 times the adjacent interspinous distance : anterior dislocation • Double appearing spinous process : Clay Shoveler's fracture • Deviation or rotation of spinous process : unilateral facet locking • Note : all these injuries have obvious signs on lateral view
AP view of patient with C2 fracture and C7 fracture-dislocation ; note rotation of spinous processes
C-Spine Trauma : Injury Mechanism Classification • Flexion • Anterior subluxation • Bilateral interfacetal dislocation • Wedge fracture vertebral body • Flexion teardrop fracture • Clay Shoveler's fracture • Extension • Central Cord Syndrome ; may have normal X-ray • Extension teardrop fracture • Hangman's fracture • Posterior atlantal arch fracture
C-Spine Trauma : Injury Mechanism Classification (cont.) • Rotation • Unilateral facet dislocation • Unilateral pillar fracture • Vertical compression • Jefferson fracture of atlas • Burst fracture of vertebral body • Odontoid fracture • Type I : (Fx of tip) : mythical (not ever seen clinically) • Type II : across base of odontoid • Type III : extends into C2 body at an angle
C-Spine Injuries : Degree of Stability A. Stable 1. Anterior subluxation 2. Unilateral facet dislocation 3. Simple wedge fracture 4. Burst fracture of lower cervical vertebrae 5. Posterior neural arch fracture of atlas 6. Pillar fracture 7. Clay-Shoveler's fracture B. Unstable 1. Bilateral facet dislocation 2. Flexion teardrop fracture 3. Extension teardrop fracture (stable in flexion, unstable in extension) 4. Hangman's fracture 5. Jefferson fracture of atlas 6. Hyperextension fracture - dislocation
Definite Signs of Unstable C-spine Injury • All anterior or posterior elements fractured • > 3.5 mm horizontal vertebral body displacement • > 11 degrees of kyphotic angulation
Incidence of Spinal Cord Injuries Occurring with Vertebral Injuries Type of Injury % with Neurologic Deficit Fracture of vertebral body only 3 Fracture of posterior elements only 19 Fracture of posterior elements and vertebral body 11 Dislocation only 17 Dislocation with fracture of posterior elements 27 Dislocation with fracture of vertebral body 56 Dislocation with fracture of posterior elements and vertebral body 61
Levels of Injury (Data from Hershey C-spine Study) Site of Fx / Dislocation C1 C2 body C2 dens C3 C4 C5 C6 C7 Number of Fractures 6 11 4 4 6 19 12 17 Total 79 Number with SCI 1 3 0 2 5 14 7 5
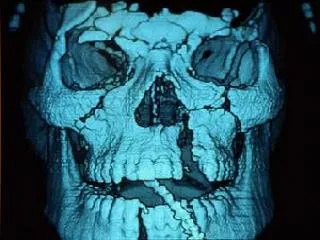
The answer to the previous question is “inadequate film” ; note that in this adequate view of the same patient, now we can see a significant fracture of C7
What injury does this film show in this patient struck on the forehead by a heavy metal beam and brought to the emergency department in cardiac arrest ?
C-Spine Trauma The Jefferson Fracture • Is a burst fracture (Fx) of the atlas • Fracture through anterior and posterior arches of C1 • Transverse atlantal ligament disrupted • Unstable • Best diagnosed on open-mouth (odontoid) view • Look for spreading of the lateral masses of C1 (the corners of the lateral masses of C1 do not line up with the corners of C2 if a Fx is present)
Lateral spread of the lateral masses of C1 with a Jefferson fracture
Conventional tomograms showing fracture of the right lateral mass and spreading of both lateral masses of C1 with a Jefferson fracture
Fracture of C1 which was only visible on this open mouth view
Coned-down view of same patient showing widened predental space (rupture of transverse atlantoaxial ligaments)