Download
1 / 28
280 likes | 321 Views
Learn how PGD, in conjunction with IVF, helps analyze embryonic cells for genetic health, enhancing chances of a successful pregnancy. Explore PGD methods and reasons for considering this advanced genetic testing.

E N D
An Introduction to:Pre-implantation Genetic Diagnosis (PGD) Mike Dougherty, Ph.D. Director of Education, ASHG
Pre-implantation Genetic Diagnosis (PGD) What is it? Genetic analysis of a single cell from an eight-cell embryo done in conjunction with in vitro fertilization (IVF) to improve the chances of a “normal” pregnancy.
The General Method of IVF • Monitor egg maturation in the ovary • Ultrasound • Hormone levels • Collect eggs (mother’s own or from donor) • - Injection of human chorionic gonadotropin (hCG) and follicle stimulating hormone (FSH) to time egg ripening • - Transvaginal aspiration using hollow needle
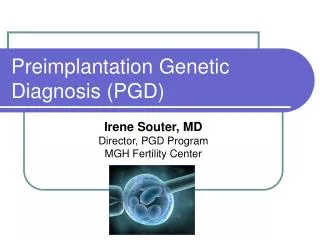
3. Obtain sperm from father (or donor) and assess quality 4. Combine eggs and sperm in vitro, using intracytoplasmic sperm injection (ICSI), if sperm is low quality 5. Nurture embryo growth by incubating in medium containing various nutrients and hormones - If doing PGD, remove one cell after 2-3 days (6-8 cell stage) for testing
An 8-cell embryo: 2-3 days zona pellucida Image adapted from and additional information can be found at: http://www.infertile.com/treatmnt/treats/pgd.htm
5. Nurture embryo growth by incubating in medium containing various nutrients and hormones - If not doing PDG, incubate until embryo is 5-6 days old (blastocyst) 6. Transfer embryos (usually 3-6) to uterus, artifically removing zona pellucida if necessary (“hatching”)
How well does IVF work? Success depends on many factors, and reliable statistics are hard to interpret because of the uniqueness of each situation and the ways in which private clinics define success.
A Sampling of Success Rates(from: Genetics and IVF Institute) The percentages shown in parentheses reference the current number divided by the number above it: The "pregnancy rate" statistics look like this:
How does this compare to natural pregnanies? It is generally accepted that a single “exposure” (copulation between fertile individuals during a period of receptivity) yields a stable pregnancy only 20-30% of the time. Failures are due to lack of fertilization, failure of the embryo to develop (often due to aneuploidy), failure to implant, menstruation.
Where would a naturally conceived embryo be during the phases of IVF development? Fertilization normally occurs in the Fallopian tubes, and the developing embryo moves through the tubes toward the uterus over a period of several days. At roughly 4-6 days, the embryo will hatch from the zona pellucida, a necessary condition for implantation in the uterine wall. Over the next week, the embryo will interact with the uterine lining in ways that stimulate placental blood flow, and development will proceed.
Why consider PGD in addition to IVF? 1. recurrent miscarriages 2. one child already affected with a genetic disease 3. family history of inherited disease 4. maternal age older than 38 5. prior failure with IVF 6. family “balancing” for sex
The Methods of Preimplantation Genetic Diagnosis • Remove a single cell from the 6-8-cell embryo using a fine glass needle to puncture the zona pellucida and aspirate the cell • In skilled hands, this generally does not harm the developing embryo. • Each cell is called a blastomere.
2. Prepare a metaphase spread of chromosomes to assess karyotype (number and integrity of each chromosome) • 3. Two types of assessment techniques are common: • a. chromosome “painting” (or FISH) using fluorescent probes specific for each chromosome. These allow number and size of each chromosome to be checked. • useful for identifying aneuploidies (incorrect chromosome numbers) and translocations • procedure destroys the tested cell • limited number of chromosomes can be checked simultaneously; some abnormalites undetectable
Fluorescence in situ hybridization (FISH) Chromosome 1 in a normal cell, “painted” with red fluorophore
Screening aneuploids with multiple probes Aneuploidy is the most frequent cause of spontaneous abortions.
Translocations may be: - “Balanced” if chromosome material merely switches locations with no net loss or gain; or - “Unbalanced” if switch is accompanied by a net loss or net gain of genetic material Balanced translocations may reduce fertility but otherwise are generally less likely to cause serious health problems. Unbalanced translocations often are harmful or lethal.
3. Two types of assessment techniques are common: • a. chromosome “painting” (or FISH) • b. genetic testing for specific disease loci (PCR or gene chips) • Polymerase chain reaction (PCR) • amplification of DNA specific to a gene of interest (family history guides choice of genes)
Examples of genetic disorders detectable via PCR-based tests: - Tay Sachs (autosomal recessive; ~98% accuracy) - Cystic fibrosis (autosomal recessive; ~85% for common allele mutation) - Huntington’s disease (autosomal dominant) - Thalassemias (autosomal recessive blood disorder) - Duchenne muscular dystrophy (X-linked recessive) - Spinal muscular atrophy As more genetic tests are developed as diagnostic tools, more will be used for predictive purposes in PDG.
Gene chip array showing expression results - Such chips allow cystic fibrosis accuracy of nearly 100% because all possible mutations can be screened.
Limitations of PCR-based tests: • Both alleles may not amplify equally, leading to misdiagnosis or inconclusive results • PCR-based tests only detect disorders at target loci; other mutations may exist elsewhere • To accommodate these limitations, prenatal amniocentesis or chorionic villus sampling is usually recommended as a supplement to PGD.
Risks of IVF to the mother/couple: • Multiple pregnancies (20-30%) • Ectopic pregnancy • Cancellation (over- or under-response to ovarian induction) • Ovarian hyperstimulation syndrome (fluid build-up in pelvic cavity due to ovarian enlargement; clotting problems) • Mechanical injury to bowel, bladder, ureters, or blood vessels during egg retrieval • Greater risk of premature delivery and delivery by Caesarean section
Risks to the child conceived via IVF/PGD: • Low birth weight; premature birth • Developmental delays • Cognitive problems (ADHD) • Urogenital problems • Cerebral pals • Certain cancers (e.g., Beckwith-Weidemann syndrome, which may be related to ICSI) • (Note: The vast majority of children born of IVF appear normal. Low birth weight, cognitive delays, and cerebral palsy are more common for any multiple-birth situation. Very few controlled, longitudinal studies have compare IVF to natural.)
What is the biological status of the embryo? At the stage of PGD, the embryo consists of 6-8 viable cells. Cells are the smallest units of life, as defined by biologists. It is generally believed that, at this stage, a single cell does not possess the potential to develop into a normal fetus. At the stage of implantation, the embryo consists of roughly 200 cells arranged in a hollow ball. Inside is an inner cell mass, the cells used to generate embryonic stem cell lines, which are cells that have the potential to develop into any tissue but not into a complete organism. Excess embryos that are not implanted are generally frozen for a time and eventually may be discarded.