Download
1 / 1
10 likes | 109 Views
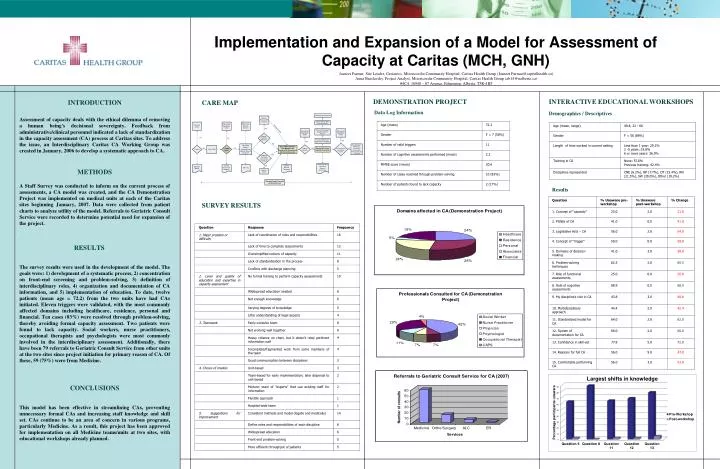
Implementation and Expansion of a Model for Assessment of Capacity at Caritas (MCH, GNH). . Jasneet Parmar, Site Leader, Geriatrics, Misericordia Community Hospital, Caritas Health Group (Jasneet.Parmar@capitalhealth.ca)

E N D
Implementation and Expansion of a Model for Assessment of Capacity at Caritas (MCH, GNH)  Jasneet Parmar, Site Leader, Geriatrics, Misericordia Community Hospital, Caritas Health Group (Jasneet.Parmar@capitalhealth.ca) Anna Braslavsky, Project Analyst, Misericordia Community Hospital, Caritas Health Group (ab14@ualberta.ca) #4C4, 16940 – 87 Avenue, Edmonton, Alberta, T5R-4H5 DEMONSTRATION PROJECT INTERACTIVE EDUCATIONAL WORKSHOPS CARE MAP Data Log Information Demographics / Descriptives INTRODUCTION Assessment of capacity deals with the ethical dilemma of removing a human being's decisional sovereignty. Feedback from administrative/clinical personnel indicated a lack of standardization in the capacity assessment (CA) process at Caritas sites. To address the issue, an Interdisciplinary Caritas CA Working Group was created in January, 2006 to develop a systematic approach to CA. METHODS A Staff Survey was conducted to inform on the current process of assessments, a CA model was created, and the CA Demonstration Project was implemented on medical units at each of the Caritas sites beginning January, 2007. Data were collected from patient charts to analyze utility of the model. Referrals to Geriatric Consult Service were recorded to determine potential need for expansion of the project. RESULTS The survey results were used in the development of the model. The goals were: 1) development of a systematic process, 2) concentration on front-end screening and problem-solving, 3) definition of interdisciplinary roles, 4) organization and documentation of CA information, and 5) implementation of education. To date, twelve patients (mean age = 72.2) from the two units have had CAs initiated. Eleven triggers were validated, with the most commonly affected domains including healthcare, residence, personal and financial. Ten cases (83%) were resolved through problem-solving, thereby avoiding formal capacity assessment. Two patients were found to lack capacity. Social workers, nurse practitioners, occupational therapists and psychologists were most commonly involved in the interdisciplinary assessment. Additionally, there have been 79 referrals to Geriatric Consult Service from other units at the two sites since project initiation for primary reason of CA. Of these, 59 (75%) were from Medicine. CONCLUSIONS This model has been effective in streamlining CAs, preventing unnecessary formal CAs and increasing staff knowledge and skill set. CAs continue to be an area of concern in various programs, particularly Medicine. As a result, this project has been approved for implementation on all Medicine teams/units at two sites, with educational workshops already planned. Results SURVEY RESULTS