Download

1 / 31
310 likes | 330 Views
ORIENTING POLICIES ON HEALTH DETERMINANTS - the process of target setting in Sweden 1985-2006 – lessons to learn Public lecture in Graz, Pallais Attems, 19.30, 8 June 2006. Bosse Pettersson Deputy Director-General. Process in 10 phases.

E N D
ORIENTING POLICIES ON HEALTH DETERMINANTS - the process of target setting in Sweden 1985-2006 – lessons to learn Public lecture in Graz, Pallais Attems, 19.30, 8 June 2006 Bosse Pettersson Deputy Director-General
Process in 10 phases • Bringing public health back on the agenda – Health for All – Alma Ata (1978) and WHO European 38 targets • Plans, programmes, plans, programmes, plans, … • Supporting and establishing regional and local capacity • Moving outside the health and medical care system – re-establishing a Swedish National institute of Public Health - SNIPH (1992) • Professional training – master programmes in public health – gradually reaching out in other sectors • The policy process and high level political involvement – the understanding of what deteremines health in contemporary societies, not to forget the historical context • Health objectives and targets set as determinants • Focus on monitoring and evaluation – indicators of determinants • Re-orienting SNIPH to become the accountable central agency (2001) • Linking public helth to equity in health and sustainable economic growth
Is there a problem? • Health in general is very good • Among the highest life expectancy in the world both for women and men • Lowest smoking rates in Europe and worldwide • Alcohol consumption just below EU average • Low accident rates, especially among childen and in road traffic • Falling death rates up to age 65 in heart diseases • Improved survival in many cancer diseases • etc
But there are old and emerging problems! • Since the 1990´s we have observed • Significant increase in sick leave, publically employed women by far the most suffering group • (Rapid?) increase in overwight and obesity among children and adolescents – decrease in physical activity • Increased alcohol consumption and mixed drinking patterns • Increase in violence related injuries • Increase in fatal fall injuries among the elderly • Self reported increase in mental ill health, especially among childdren, adolecscents and women • Falling health life expectancy among women 45+ and older
In general …mixed progress and failure • Health is improving in absolute terms for most people, but • for the least priveliged groups significantly slower • in relative terms health inequalities are increasing • Life expectancy beween municipalities and socio-economic status can differ up to approximately 6 years among Swedish men!
Is there anything to do? • Peoples’s well-being can be improved by health promotion • 85-90 per cent of the Swedish disease burden is caused by non communicable and/or chronic disesases, where premature deaths and disabilities can be prevented • Inequalities in health are not cased by chance – the origin from systematic social unjustice
... and, if nothing is done …? • The next generation may be the first in modern times to experience shorter lives than their parents • It will pose a serious threat against the affordability of any well developed social welfare system • It has the potential to create unforseen political tensions in our societies – health is becoming an issue of security
The Swedish National Public Health Institute – SNIPH (1) • Re-established 1992 (originally founded/operating 1938-1968) for implemenation of prioritized health promotion and disease prevention programmes • Re-oriented 2001 to have a central position in facilitating, implementing, co-ordinating monitoring and evalution and further development of the national public health strategy • Directly under the Ministry of Health and Social Affairs • since 2002 a special Public Health Cabinet Minister
The Swedish National Public Health Institute – SNIPH (2) Staffing and financial resources • 160 staff • Annual budget 2006 – almost 100% tax funded (1 € = 9,4 SEK) • General 136 million SEK ~ € 14,5 mill • Note: In addition,special funding for prevention of hiv/aids, illicit drugs and harmful alcohol consumption
Not alone – state level • Besides SNIPH • National Board of Health& Welfare • Swedish Institute for Infectous Diseases Control (SMI) • Swedish Medical Products Agency • The National Social Insurance Board • Swedish Work Environment Authority • National Institute for Working Life • Research Councils (funding) and institutions
Not starting from ZERO - building bricks in the Swedish public health strategy Modern public health and WHO’s Health for All’ fir for purpose • Longstanding commitment across political parties – although different emphasis and ideologies • Evolved as a concern on all political levels – but, the regional a forerunner • Infra-structures for ‘modern public health’ gradually in place from the 1980´s; state seed money speeded up the development
1. Historical • Long tradition of public health outside the medical sector since 17th century • Church • Popular movements • Public health institute est. 1938
2. Contextual [1] – autonomous regional and local levels – WHERE PEOPLE ARE AT! • 21 County Councils/Regions (political) • All with community medicine/public health units, but mainly focusing on health and medical care • 290 municipalities (political) • App. 75-80 per cent with local health planners, policies and programmes
2. Contextual [2] – local level • Municipalities the 3rd autonomous political level. • Initially health protection • Social welfare responsibility – increasingly linked to health • Health promotion concept better understood than disease prevention
Professional training – MPH programmes critical to skilled workforce • Piloting started on national level in 1988 • Established during the 1990‘s • Still increasing interest • 14 universities & university colleges with MPH programmes (Complete or partial) • Well educated workforce in modern public health • Emerging employment opportunities
Why determinants as ‘objectives and targets’? • Politicians cannot directly prevent deaths and illness in cancer, nor heart diseases etc, but can influence what is behind – the ‘upstream approach’ • Inequalities overall priority
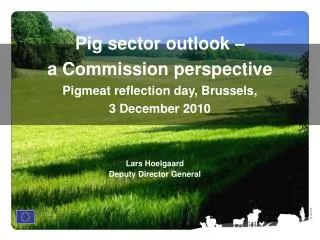
Environment Public economic strategies Educa- tion Agri- culture & food- stuff Traffic Leisure & culture Social- insurance Eatinghabits Social assistance Social network Employ- ment Alcohol Age, sex, heredity Health-& medical care Sleep habits Social support Contact children and adults Work environment Tobacco Sex & life together Physical activity Illicit drugs Housing Haglund, Svanström, KI, revision, Beth Hammarström
Model for national public health strategy – the principal foundation National public health objective domains Health determinants Health outcomes & distribution Inter- ventions Bosse Pettersson, 2003
Model for national public health strategy – the links National public health objective domains Health determinants Health outcomes & distribution Impact & efficiency Correlation Inter- ventions ’Upstream approach’ Bosse Pettersson, 2003
One overall national public health aim • “ To create social conditions that will ensure good health for the entire population”. • Equity perspective on health. • To be achieved by implementing initiatives in 31 national policy areas related to 11 objectives.
11 public health objectives • Participation and influence in society. • Economic and social security. • Secure and favourable conditions during childhood and adolescence. • Healthier working life. • Healthy and safe environments and products. • A more health promoting health service. • Effective prevention against communicable diseases. • Safe sexuality and good reproductive health. • Increased physical activity. • Good eating habits and safe food. • Reduced use of tobacco and alcohol, a society free from illicit drugs and doping and a reduction in the harmful effects of excessive gambling.
One overarching aim: To provide societal conditions for good health on equal terms for the entire population 11 Objective domains in brief 9-11: Physical activity -Eating habits and safe food -Tobacco, alcohol, illicit drugs, doping, harmful gambling Lifestyles and health behaviours 4-8: Healthier working life – Sound and safe environments & products – A more health promoting health care system – Effective protection against communicable diseases – Safe sexuality and a good reproductive health Settings and environments 1- 3: Participation and influence on the society – Economic and social security – Safe and favorable growing up conditions Societal structures and living conditions Bosse Pettersson, 2003
How to make it work? • a special Minister of Public Health appointed + National high-level Steering Committee • sectoral responsibilities defined for more than 30 national agencies by existing political domain objectives • public health integrated into ‘daily business’ – existing sectoral objectives and targets influencing health
Implementation by monitoring & evaluation INDICATORS • for monitoring and evaluation the policy • to be agreed by involved state agencies, and negotiated with local municipalities and regional County Councils • to form the base for the new Public Health Policy Report, to be delivered by the Government to the Parliament once each 4th year, first in 2005
Demands on indicators • Strong correlation to health. • Strong validity for the determinant. • Meaningful and possible to change by political decisions. • Be relatively inexpensive to admininstrate. • Stratified by sex, age, type of family, different geographical levels (including the municipal level), socio-economic group and ethnicity where possible. Bernt Lundgren 2004
Monitoring and evaluation of public health strategy Public Health Policy report Health determinants Health outcomes & distribution Impact & efficiency Correlation Inter- ventions Info Population Health report etc Monitoring & evaluation system Indicators Bosse Pettersson, 2003
The Swedish National Public Health Institute – SNIPH (2) Remit – 3 major missions • Monitoring and evaluation of the public health strategy and facilitate its implementation • Centre of knowledge for effective health promotion and disease prevention methods • Overall supervision of selective preventive legislation in the fields of alcohol and tobacco
Tools for implementation • Determinant’s indicators with inequality and gender dimensions • Governmental directives to concerned sectoral state agencies • Health Impact Assessment (HIA) recognized • Datasets and planning tools for reviewing and integration public health at local municipal level are elaborated • Basic municipal public health data on the web • Local Welfare Management Systems (LOWEMANS)
Shortcomings and criticism • to vague, determinants are difficult to explain • to small resources allocated for general public health infrastructures • Intervention research is lacking • need training of exiting professionals in concerned sectors • lack of funding to municipalities and county councils where major efforts are expected to take place
Good practices work • traffic accidents; speed limits, road construction, safe vehicles, bicycle helmets • high taxes on alcohol reduces health related harm • comprehensive tobacco prevention reduces smoking incidence and related illness and premature deaths
Public health – increasingly a global and international matter • EU • Public Health Programme • Health inequalities • Health in other policies; agriculture • WHO • Strengthen public health dimension – MDG’s • Non-communicable diseases • Alcohol • Diet & physical exercise • Tobacco • Reproductive and maternal & child health • Mental health • Health Promotion – Bangkok Charter • HIV/aids