Download
1 / 18
210 likes | 989 Views
SYNDROME OF INAPPROPRIATE SECRETION OF ANTIDIURETIC HORMONE (SIADH). BACKGROUND. A variety of disorders are associated with plasma ADH concentrations Thus, water retention accompanies normal water intake, leading to hyponatremia and hypo-osmolality.

E N D
SYNDROME OF INAPPROPRIATE SECRETION OF ANTIDIURETIC HORMONE (SIADH)
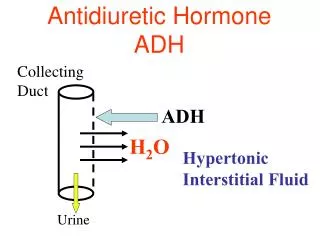
BACKGROUND • A variety of disorders are associated with plasma ADH concentrations • Thus, water retention accompanies normal water intake, leading to hyponatremia and hypo-osmolality. • The urine is usually more concentrated than plasma . • Termed the syndrome of inappropriate secretion of antidiuretic hormone, or SIADH. • The clinical picture can be produced experimentally by giving high doses of vasopressin to a healthy subject receiving normal to high fluid intake. • Water restriction in patients suspected of having SIADH will result in plasma osmolality and sodium concentration returning to normal.
The diagnostic criteria • The diagnostic criteria for SIADH include • (1) hyponatremia with corresponding plasma hypo-osmolality (< 280 mosm/kg); • (2) urine less than maximally dilute, ie, inappropriately concentrated (> 100 mosm/kg); • (3) euvolemia (including absence of congestive heart failure, cirrhosis, and nephrotic syndrome); • (4) absence of renal, adrenal or thyroid insufficiency. Urinary sodium is usually > 20 mmol/d, probably a consequence of increased atrial natriuretic factor. Dynamic testing and plasma ADH levels are usually unnecessary in diagnosis.
Causes of SIADH - Malignant lung disease, particularly bronchogenic carcinoma- Nonmalignant lung disease, eg, tuberculosis- Tumors at other sites (especially lymphoma, sarcoma), eg, duodenum, pancreas, brain, prostate, thymus- Central nervous system trauma and infections- Drugs that stimulate vasopressin release, eg, clofibrate, chlorpropamide, and other drugs such as thiazides, carbamazepine, phenothiazines, vincristine, cyclophosphamide SSRIs (eg, fluoxetine, sertraline)- Endocrine diseases: adrenal insufficiency, myxedema, anterior pituitary insufficiency- HIV infection
Types of Osmoregulatory Defects • Type A: - Found in 20% of patients, - Characterized by large irregular changes in plasma ADH completely unrelated to serum osmolality. - Associated with both malignant and nonmalignant disease.
Types of Osmoregulatory Defects • Type B: - Found in about 35% of patients - Associated with secretion of ADH that is excessive but proportionate to osmolality. - In these patients, the osmotic control of ADH secretion appears to be either set at a low level or abnormally sensitive to changes in serum osmolality.
Types of Osmoregulatory Defects • Type C: - Found in 35% of patients, - Characterized by a high basal level of ADH that rises even higher with a rise in serum osmolality.
Types of Osmoregulatory Defects • Type D: - Found in only 10% of patients, represents a different type of problem. - ADH is normally suppressed in hypovolemic states and rises normally with increase in osmolality. - Thus, the SIADH in these patients may be associated with a change in renal sensitivity to serum arginine vasopressin.
LÂM SÀNG • SIADH là nguyên nhân thường gặp của hạ Na máu • TCLS của hạ Na máu liên hệ đến TKTU • TCLS sớm của hạ Natri máu là chán ăn, buồn ói, lơ mơ và vô cảm, • Nặng hơn là mất định hướng, kích động,kinh giật,giảm PX,TC thiểu năng TKVĐ và đôi khi có nhịp thở Cheyne-Stocks • Hôn mê và động kinh khi Na<120mEq/L • Hạ Na máu mãn,Na>125mEq/L ít có TCLS • Na<105mEq/L: ½ số BN sẽ chết • TCLS ít liên quan với nồng độ Na , nhưng liên quan nhiều với tốc độ giảm Na máu
LÂM SÀNG • Khi áp lực thẩm thấu HT trở lại bình thường TC sẽ đảo ngược • Tuy nhiên, nếu điều trị quá nhanh có thể gây ly giải myelin vùng cầu của TKTU liệt mềm, nói khó, nuốt khó
Treatment • The treatment of SIADH depends upon the underlying cause. • A patient with drug-induced SIADH is treated by withholding the drug. • The treatment of SIADH in a patient with bronchogenic carcinoma is more complicated, however, and the prognosis is poor. • Treatment aims to return plasma osmolality to normal without causing further expansion of the extracellular fluid compartment, as would occur following infusion of hyperosmotic solutions.
Treatment • A. FLUID RESTRICTION • The simplest form of treatment is fluid restriction, although in the long term the excessive thirst associated with this treatment may be difficult to manage
Treatment • B. DIURETICS • If plasma osmolality is low loop diuretics such as furosemide can be employed. • These agents limit free water generation in the loop of Henle and reduce the concentration gradient in the renal medulla • Because diuresis is accompanied by significant urinary losses of potassium, calcium, and magnesium, these electrolytes should be replaced by intravenous infusion
Treatment C. OTHER METHODS • Severe hyponatremia: hypertonic saline, ie, 3% saline IV 0.1 mL/kg/min. However fluid overload may precipitate heart failure or circulatory collapse, and overly rapid correction may lead to central pontine myelinolysis. • Drugs that reduce the effect of vasopressin on the kidney may be useful. - Demeclocycline, 1-2 g/d orally, causes a reversible form of nephrogenic diabetes insipidus. However, it is nephrotoxic, and renal function (blood urea nitrogen and serum creatinine) must be monitored carefully. - Lithium carbonate has a similar effect, but therapeutic doses are so close to the toxic dose that this drug is rarely useful
Tài liệu tham khảo 1. Nội tiết học đại cương – Mai Thế Trạch, Nguyễn Thy Khuê 2. Williams Textbook of Endocrinology, 11th 3. Basic & Clinical Endocrinology, 7th Edition