Download
1 / 72
720 likes | 961 Views
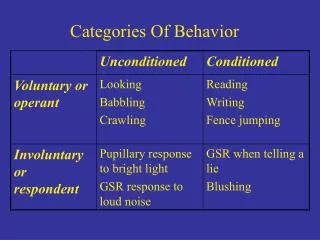
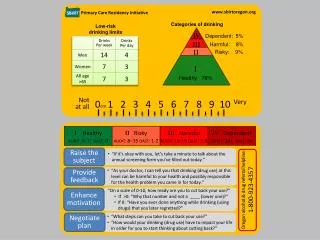
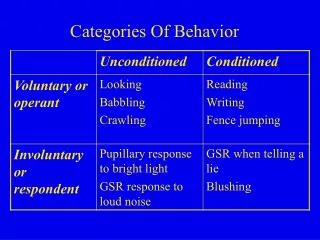
Categories of Volume Disorders. Intravascular/acute hemorrhage Extracellular Intra- and extravascular Sodium and water loss Diarrhea Sodium and water gain CHF with edema Ascites Total body water Water loss Diabetes insipidus Water retention SIADH. Diagnosis of Volume Disorders.

E N D
Categories of Volume Disorders • Intravascular/acute hemorrhage • Extracellular • Intra- and extravascular • Sodium and water loss • Diarrhea • Sodium and water gain • CHF with edema • Ascites • Total body water • Water loss • Diabetes insipidus • Water retention • SIADH
Diagnosis of Volume Disorders • Intravascular depletion • MAP = CO × SVR • Clinical signs • BP HR JVP • Cool extremities • Reduced sweating • Dry mucous membranes • ECF Depletion • Skin turgor • Weight • Hemodynamic effects
Hemodynamic Truths • Tachycardia is never a good thing. • Hypotension is always pathologic. • There is no such thing as normal cardiac output. • Central venous pressure is only elevated in disease. • Peripheral edema is of cosmetic concern Pinsky.. Chest. 2007; 132:2020-2029)
Distribution of Total Body Water Intracellular 25L K Interstitial 12 L Na Plasma 3 L Protein Total Body Water (40 L) ECF (15 L)
Daily Fluid Balance Intake 1-1.5 L (100-200 mEq Na+) Total Body Water Insensible losses 200 ml/day/m2 BSA Sweat 0.1 L (6 mEq Na+) Urine 1-1.5 L (100-200 mEq Na+)
Principles of Treatment • How much volume? • Need to estimate volume deficit • Which fluid? • Which compartment is predominantly effected? • Evaluate acid-base status, electrolytes and nutrition
Case 1 A 56 y.o. male presents with massive hematemesis. PE: Diaphoretic BP supine 120/70 HR 100 BP sitting 90/50 HR 140 Serum Na+ 140 What is the nature of the volume deficit? What IV fluid would you prescribe?
Case 2 An 28 y.o. intern returns from the intern beach weekend with intractable nausea and vomiting. PE: BP 80/50 HR 130 supine Labs: Na+ 130 K+ 2.8 HCO3- 32 What is the nature of the fluid deficit? What would happen if D5W were administered?
Case 3 An 85 y.o. nursing home resident with dementia and a history of diabetes presents with confusion. PE: BP supine 110/70 90/50 sitting. Decreased skin turgor. Wt 60 kg Labs: Na+ 150 Glucose 1200 BUN 50/Creat 1.8 How would you treat this patient?
Calculation of Water Deficit Na × Normal body water = Na × Current body water 140 × NBW = 157 × (0.5 X 60 kg) NBW = 33.6 L Water deficit = 33.6 L -30 L = 3.6 L
Case 4 A 40 y.o. patient with cirrhosis and ascites is admitted with a rising creatinine. BP 100/70 JVP 5 cm Tense ascites No edema BUN 12 Creat 2 Albumin 2 Urine Na 5 mEq/L Urine volume 200 mL/24 hours If volume depleted, how would you treat the patient?
Case 5 A 76 y.o. male with COPD is admitted for a COPD exacerbation. Oral intake over the first day of hospitalization has been poor. PE Euvolemia Na 140 K 3.8 BUN 13 Creat 1 What would you choose for maintenance fluids?
Chronic Hyponatremia: Epidemiology • Most common electrolyte disorder, occurring in 15-30% of hospitalized patients • SIADH accounts for 60% of cases of chronic hyponatremia
Incidence of Hyponatremia Nephrol Dial Transplant 21: 70-76, 2006.
Symptomatic Hyponatremia Per cent of Patients with Symptomatic Hyponatremia • 27,496 Outpatients • 14% with • SNa <134 mEq/L • 4% SNa < 130 mEq/L J Am Soc Nephrol 16: 531A, 2005.
Diagnostic Evaluation of Hyponatremia >290 Hypertonic Hyponatremia (Hyperglycemia) Effective Plasma Osmolality (2×Na + glucose/18) Measured Osm 275-290, Na+ < 135 & BUN Normal < 275 mOsm/kg True Hyponatremia Pseudohyponatremia Edematous Effective Volume Euvolemic Volume Depleted Uosm >100 mosm/kg Uosm >100 mosm/kg Uosm >100 mosm/kg Uosm <100 mosm/kg UNa < 15meq/L (Exceptions) UNa > 25 meq/L UNa < 15meq/L UNa < 15meq/L CHF Cirrhosis Nephrosis True Volume Depletion SIADH Exclude hypothyroidism and adrenal insufficiency Primary Polydipsia Low Solute Intake
Pseudohyponatremia N Engl J Med 349: 1465-1469, 2003.
SIADH ADH Water Restrict 140 SNa+ mEq/L 120 1000 Uosm mOsm/kg 50 200 UNa+ mEq/L 0 17 ECF Vol L 15 0 2 4 6 8 10 12 14 16 18 Days
SIADH versus Volume Depletion Favors SIADH Serum Uric Acid < 4 mg/dL FexUA > 10% BUN < 5 mg/dL FexUN > 70% Favors Volume Depletion Serum Uric Acid > 6 mg/dL FexUA < 10% BUN > 15 mg/dL FexUN < 35% • Response to 1-2 liters of 0.9% NaCl in patients who are • not symptomatic
Causes of SIADH CNS Disorders Acute psychosis Hemorrhage Inflammatory and demyelinating diseases Mass lesions Stroke Trauma Pulmonary Disorders Acute respiratory failure Infections Positive-pressure ventilation Tumors Extrathoracic Mediastinal Pulmonary Vigorous exercise SIADH Miscellaneous HIV infection Pain Postoperative state Nausea Drugs Carbemazepine Oxytocin Clofibrate Phenothiazines Cyclophosphamide NSAID’s, Cox-2 I’s Desmopressin SSRI’s Nicotine Tricyclics Opiates Vincristine Methylenedioxymethamphetamine (Ecstacy)
Treatment of Hyponatremia • Treat symptomatic patients with 3% saline (and furosemide) • Stop therapy with 3% saline when symptoms resolve • Do not exceed 10 mEq/L in 24 hours or 18 mEq/L in 48 hours in a symptomatic patient with chronic hyponatremia • Use 0.9% NaCl for asymptomatic hyponatremia due to volume depletion • Do not use fluid restriction alone in patients with symptoms of brain edema • Do not use 0.9% NaCl for symptomatic patients with SIADH, especially when the urine osm is > 300 mOsm/kg • Stop offending drugs whenever possible
Assessment of Renal Function –The MDRD Equation • GFR should be estimated by the MDRD equation in most circumstances • Should be applied to patients in a steady state with respect to serum creatinine concentration • not valid in the setting of a rising serum creatinine in acute kidney injury (AKI) • Less accurate in populations with normal or near normal GFR, extremes of age and weight, amputees, in pregnancy and cirrhosis • Measure creatinine clearance in these populations
MDRD Equation GFR in mL/min per 1.73 m2 = 175 x Cr(exp[-1.154]) × Age(exp[-0.203]) × (0.742 if female) x (1.21 if black) www.kidney.org/professionals/KLS/gfr_calculator.cfm www.nephron.com/mdrd/default.htm
Serum Creatinine (SCr) Alone Is a Poor Indicator of Kidney Function 2 patients with SCr levels of 1.5 mg/dL (0.133 mmol/L) Male Age = 25 years FemaleAge = 65 years Estimated GFR*: 73 mL/min Estimated GFR*: 37 mL/min • *Calculated with the MDRD equation.
Problem with Serum Creatinine in Estimating GFR Creatinine 0.5 mg/dL (0.044 mmol/L) to 0.8 mg/dL (0.071 mmol/L) GFR 100 to 60 mL/min
Cystatin C • More sensitive in identifying milder impairments in renal function than serum creatinine • Cystatin C-based equations may more accurate in the elderly and in patients with cirrhosis • Levels are affected by thyroid status, inflammation, and corticosteroids • Clinical utility remains to be established
Key Points • The estimated GFR should be calculated using the MDRD equation whenever a serum creatinine is measured in steady state conditions • Plots of GFR vs. time are helpful in patient management and education • Consider 24 hour urine collections for creatinine clearance in the following populations: • Near normal GFR • Extremes of age and weight • Amputees • Pregnant women • Cirrhotics
Etiology of Hospital Acquired AKI Nash K, et al. AJKD 2002; 39: 930-936.
Medication-Induced AKI in Hospitalized Patients Nash K et al. AJKD 2002; 39: 930-936.
Acute Kidney Injury • Prevalence • 1% all patients admitted to hospital • 10-30% patients admitted to ICU • Etiology • Hemodynamic 30% • Parenchymal 65% • Acute tubular necrosis 55% • Acute glomerulonephritis 5% • Vasculopathy 3% • Acute interstitial nephritis 2% • Obstruction 5%
Evaluation of Renal Failure • Is the renal failure acute or chronic? • laboratory values do not discriminate between acute vs. chronic • oliguria supports a diagnosis of acute renal failure • small kidneys on US more common in chronic renal failure • What is the etiology of the renal failure? • Prerenal 30% • Intrarenal 65% • Postrenal 5%
5 Key Steps in Evaluating Acute Kidney Injury • Obtain a thorough history; review the chart in detail • Do everything you can to accurately assess volume status • Always order a renal ultrasound • Look at the urine • Review urinary indices
Clinical Approach to Acute Kidney Injury History Volume status Ultrasound Urinalysis US shows Hydronephrosis Urinalysis Normal Urinalysis Abnormal Post-Renal Pre-renal Tubulointerstial Disorders Glomerular and Vascular Disorders
Clinical Approach to Acute Kidney Injury History Volume Status Ultrasound Urinalysis Hydronephrosis Normal Urinalysis Pre-Renal Vascular Disorders Urinalysis abnormal Post-Renal Low ECF Volume GI losses Hemorrhage Diuretics Osmotic diuresis Altered renal blood flow or hemodynamics Sepsis Heart failure Cirrhosis/Hepatorenal syndrome Hypercalcemia Medications NSAIDs/Cox-2 inhibitors ACE inhibitors Angiotensin II receptor blockers Vascular disease Prostate disease BPH Cancer Pelvic malignancy Stones Stricture Retroperitoneal fibrosis Arterial Renal artery stenosis Renal artery thromboembolism Fibromuscular dysplasia Takayasu arteritis Medium vessel Polyarteritis nodosa Kawasaki disease Small vessel Glomerulonephritis Thrombotic microangiopathies Cholesterol emboli Renal vein Renal vein thrombosis Abdominal compartment syndrome Renal parenchymal disorders Glomerular Disorders Tubulointerstitial Disorders Tubular obstruction Crystals Calcium oxalate (Ethylene glycol, orlistat) Indinivir Acyclovir Methotrexate Tumor lysis syndrome Myeloma cast nephropathy Acute tubular necrosis Ischemic Nephrotoxic Contrast-induced Rhabdomyolysis Acute interstitial nephritis Medication-induced Autoimmune Sjogren syndrome Sarcoidosis Infection-related
Pre-renal Azotemia History Effective Arterial Volume Normal Renal Ultrasound Normal Urinalysis Low ECF Volume GI losses Hemorrhage Diuretics Osmotic diuresis Altered renal blood flow or hemodynamics Sepsis Heart failure Cirrhosis/Hepatorenal syndrome Hypercalcemia Medications NSAIDs/Cox-2 inhibitors ACE inhibitors Angiotensin II receptor blockers Vascular disease
Acute Kidney Injury in the ICU Decreased Effect Renal Blood Flow Sepsis Systemic inflammation Impaired cardiac output Nephrotoxins Aminoglycosides Amphotericin Foscarnet Rhabdomyolysis Iodinated radiocontrast Pre-renal Azotemia Nephrotoxic tubular injury Ischemic tubular injury Acute tubular necrosis
ATN versus Prerenal Azotemia Indices Prerenal ATN UNa < 20 > 40 FeNa < 1% > 4% U/PCreat > 40 < 20 FeUN < 35% >70%
Urine Sediment Abnormal Pre-renal Post-renal Normal WBC WBC Casts Eosinophils RTE cells Pigmented casts RBC RBC Casts Proteinuria Glomerulonephritis Vasculitis Thrombotic microangiopathy Atheroemboli Tubular Epithelial Injury -ischemic -nephrotoxic aminoglycoside rhabdomyolysis Pyelonephritis Interstitial nephritis Allergic IN Atheroemboli Glomerulonephritis
Urinalysis Findings in Acute Kidney Injury Urinary Sediment Diagnosis Urine Dipstick Dysmorphic Hematuria Red cell casts 3+ protein Glomerulonephritis Minimal change disease Focal segmental glomerulosclerosis Oval fat bodies Fatty Casts Acute tubular necrosis 1+ protein Muddy brown casts Renal tubular epithelial cells and casts Acute interstitial nephritis Urinary tract infection Minimal abnormalities (few cells, minimal protein) White cells White cell casts Eosinophiluria Cholesterol emboli Thrombotic microangiopathy +Blood on dipstick with no RBCs on microscopic Pigment nephropathy (Rhabdomyolysis with ATN) Drug toxicity Urate crystals/calcium-phosphate crystals -tumor lysis syndrome Calcium oxalate crystals -ethylene glycol -orlistat Crystalluria Monomorphic Hematuria Obstructing stone Obstructing tumor Renal vein thrombosis Renal infarction -Protein on dipstick with +Sulfasalicylic acid assay for protein Myeloma cast nephropathy
Key Points on Medication-induced AKI • Medications are the second most common cause of cause of AKI in hospitalized patients (pre-renal azotemia is #1) • THINK DRUGS • NSAIDs can result in significant nephrotoxicity in the elderly, and in patients with diabetes and/or CKD • Consider AIN in patients on PPI’s with unexplained kidney injury and pyuria • Use of oral phosphasoda preparations for bowel prep should be abandoned-use PEG based preps
Renal Biopsy-When? • Exclude pre- and post-renal failure, and clinical findings are not typical for ATN • Extra-renal manifestations that suggest a systemic disorder • Heavy proteinuria • RBC casts
Tumor Lysis Syndrome • Acute oliguric renal failure associated with urate levels > 15 mg/dl and hyperphosphatemia • Associated with overproduction and excretion of urate and cell lysis resulting in increased release of potassium and phosphorus in patients undergoing chemotherapy or with a heavy tumor burden • Urine urate/creatinine > 1 • Urinary alkalinization may worsen calcium phosphate precipitation and NS is as effective as urinary alkalinization alone • Early dialysis indicated for oliguric AKI to decrease urate burden
Risk Stratification for TLS *From Coiffier B, Altman A, Pui CH, Younes A, Cairo MS. Guidelines for the management of pediatric and adult tumor lysis syndrome: an evidence-based review. J Clin Oncol. 2008; 26:2767-78.
Prevention of TLS • If there is a concern about tumor lysis, as predicted by an elevated serum LDH, serum uric acid, or heavy tumor burden, the patient should be admitted for hydration and close monitoring of kidney function, serum potassium, phosphorus and uric acid. • Patients with a preexisting reduction in GFR, oliguria and/or acidic urine, and volume depletion should also be hospitalized for hydration and observation. • High-risk patients should be hospitalized for aggressive intravenous hydration and prophylactic rasburicase. • Intermediate risk patients should receive allopurinol rather than rasburicase for prophylaxis in the absence of pretreatment hyperuricemia. • Patients at low risk for TLS should receive hydration, but do not require hypouricemic therapy.
Renal Disease Associated with Multiple Myeloma • Myeloma cast nephropathy • direct precipitation of casts in tubules • Factors favoring cast precipitation: -affinity of light chains for Tamm-Horsfall protein -high luminal Cl- -volume depletion • Plasmapheresis may be beneficial • Hypercalcemic nephropathy • Glomerular lesions (MPGN, Amyloid, Light chain deposition disease)
Acute Glomerulopathies • RPGN most commonly seen with: • Lupus nephritis (DPGN, class IV) • Pauci-immune GN (ANCA associated) • Anti-GBM disease • less commonly: IgA, post-infectious • Nephrotic presentations of ARF • Collapsing FSGS (HIV nephropathy) • Minimal change disease with ATN • Thrombotic microangiopathies (HUS, TTP, malignant hypertension, scleroderma kidney, pre-eclampsia)
Atheroembolic Renal Disease • ARF in patient with erosive atherosclerosis • Often follows aortic manipulation (angiography, surgery, trauma) or anticoagulation • Pattern is often an acute worsening of renal function due to showering of emboli, followed by more insidious progression over several weeks to months due to ongoing embolization of atheromatous plaques • Livedo reticularis, Hollenhorst plaques • Nephritic sediment, eosinophilia, eosinophiluria, low C3 • Poor prognosis