Download
1 / 1
10 likes | 155 Views
Severe Left Heart Obstruction Importantly Influences Fetal Cerebral Blood Flow. Yuka Yamamoto, Paul Brooks, Nee Khoo, Akiko Hirose and Lisa K Hornberger.

E N D
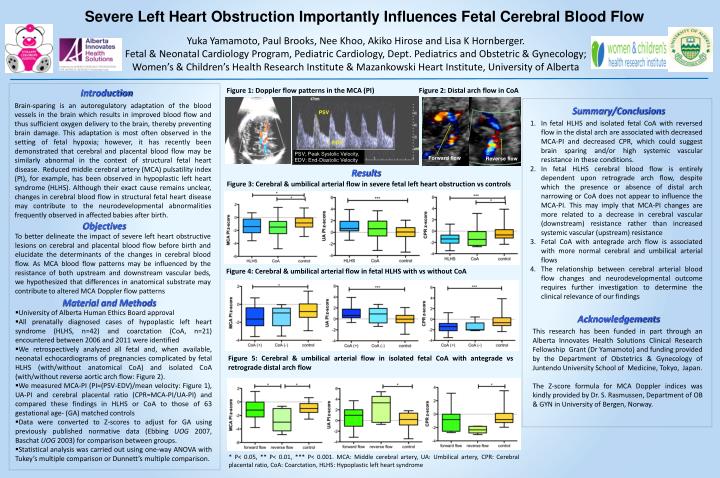
Severe Left Heart Obstruction Importantly Influences Fetal Cerebral Blood Flow Yuka Yamamoto, Paul Brooks, Nee Khoo, Akiko Hirose and Lisa K Hornberger. Fetal & Neonatal Cardiology Program, Pediatric Cardiology, Dept. Pediatrics and Obstetric & Gynecology; Women’s & Children’s Health Research Institute & Mazankowski Heart Institute, University of Alberta Figure 1: Doppler flow patterns in the MCA (PI) Figure 2: Distal arch flow in CoA Introduction Brain-sparing is an autoregulatory adaptation of the blood vessels in the brain which results in improved blood flow and thus sufficient oxygen delivery to the brain, thereby preventing brain damage. This adaptation is most often observed in the setting of fetal hypoxia; however, it has recently been demonstrated that cerebral and placental blood flow may be similarly abnormal in the context of structural fetal heart disease. Reduced middle cerebral artery (MCA) pulsatility index (PI), for example, has been observed in hypoplastic left heart syndrome (HLHS). Although their exact cause remains unclear, changes in cerebral blood flow in structural fetal heart disease may contribute to the neurodevelopmental abnormalities frequently observed in affected babies after birth. Summary/Conclusions • In fetal HLHS and isolated fetal CoA with reversed flow in the distal arch are associated with decreased MCA-PI and decreased CPR, which could suggest brain sparing and/or high systemic vascular resistance in these conditions. • In fetal HLHS cerebral blood flow is entirely dependent upon retrograde arch flow, despite which the presence or absence of distal arch narrowing or CoA does not appear to influence the MCA-PI. This may imply that MCA-PI changes are more related to a decrease in cerebral vascular (downstream) resistance rather than increased systemic vascular (upstream) resistance • Fetal CoA with antegrade arch flow is associated with more normal cerebral and umbilical arterial flows • The relationship between cerebral arterial blood flow changes and neurodevelopmental outcome requires further investigation to determine the clinical relevance of our findings PSV; Peak Systolic Velocity, EDV; End-Diastolic Velocity Results Figure 3: Cerebral & umbilical arterial flow in severe fetal left heart obstruction vs controls Forward flow Reverse flow Objectives To better delineate the impact of severe left heart obstructive lesions on cerebral and placental blood flow before birth and elucidate the determinants of the changes in cerebral blood flow. As MCA blood flow patterns may be influenced by the resistance of both upstream and downstream vascular beds, we hypothesized that differences in anatomical substrate may contribute to altered MCA Doppler flow patterns Figure 4: Cerebral & umbilical arterial flow in fetal HLHS with vs without CoA Material and Methods • University of Alberta Human Ethics Board approval • All prenatally diagnosed cases of hypoplastic left heart syndrome (HLHS, n=42) and coarctation (CoA, n=21) encountered between 2006 and 2011 were identified • We retrospectively analyzed all fetal and, when available, neonatal echocardiograms of pregnancies complicated by fetal HLHS (with/without anatomical CoA) and isolated CoA (with/without reverse aortic arch flow: Figure 2). • We measured MCA-PI (PI=(PSV-EDV)/mean velocity: Figure 1), UA-PI and cerebral placental ratio (CPR=MCA-PI/UA-PI) and compared these findings in HLHS or CoA to those of 63 gestational age- (GA) matched controls • Data were converted to Z-scores to adjust for GA using previously published normative data (Ebbing UOG 2007, Baschat UOG 2003) for comparison between groups. • Statistical analysis was carried out using one-way ANOVA with Tukey’s multiple comparison or Dunnett’s multiple comparison. Acknowledgements This research has been funded in part through an Alberta Innovates Health Solutions Clinical Research Fellowship Grant (Dr Yamamoto) and funding provided by the Department of Obstetrics & Gynecology of Juntendo University School of Medicine, Tokyo, Japan. The Z-score formula for MCA Doppler indices was kindly provided by Dr. S. Rasmussen, Department of OB & GYN in University of Bergen, Norway. PSV Figure 5: Cerebral & umbilical arterial flow in isolated fetal CoA with antegrade vs retrograde distal arch flow EDV * P< 0.05, ** P< 0.01, *** P< 0.001. MCA: Middle cerebral artery, UA: Umbilical artery, CPR: Cerebral placental ratio, CoA: Coarctation, HLHS: Hypoplastic left heart syndrome