Download
1 / 24
240 likes | 302 Views
Discusses GBS as a cause of neonatal infection & identifies other pathogens impacting neonatal health, with focus on a case study and cohort study methodology.

E N D
Changing Epidemiology of Bacteraemia in Infants aged 1 week to 3months Mekhala Ayya SCH Journal Club 3rd April 2014 TL Greenhow, Yun-Yi Hung, Arnd M Herz
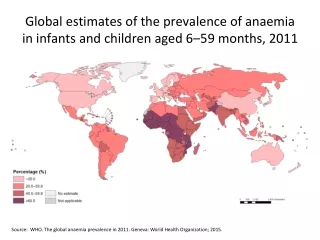
Aims To determine if GBS is still one of the main causes of neonatal infection To identify other pathogens that can cause neonatal infection
Objectives Select an appropriate paper from the literature Discuss the paper’s methodology and findings Look at what this paper adds to our knowledge Should we change our practice?
Case 11 day old baby Born at Term ( 40+4) Birth weight of 3.65kg Not gaining weight Good oral intake but mum felt that he was generally more grizzly than usual ( for 3 days) Non Specific symptoms CRP> 200 Received full septic screen, blood cultures negative
The Clinical Question • Population Infants aged 1 week – 3 mths with clinical suspicion of infection • Intervention Infants with positive blood cultures • Comparison Infants with negative blood cultures • Outcome Survival/Morbidity/Hospital Stay Identify the common pathogens • Design Cohort study
Literature Search • Late onset neonatal sepsis • Bacteraemia • Septic screen • Limited search to Neonates and Infant aged < 23 3months • Searched Medline, EMBASE and Trip Database • Limited to English Language
Search Results and Article Selection • Multiple articles – mainly regarding the management and diagnostic techniques in infants < 3mths with suspected infection • Article selected as: • Most recent • From presentation • In keeping with my case and clinical question regarding pathogens
Current Practice In infants < 3 mths Clinical suspicion of infection Low threshold for performing a full septic screen
Methodology • Cohort Study • Retrospective identification of positive blood culture in infants ages between 1 week to < 3mths of age • Full Term infants ( >37 weeks gestation) • January 1st 2005 – December 31st 2009 • Diagnosis of bacteraemia ( likely pathogen)
Methodology Continued • Review of computerised medical records database • Contained all blood cultures results of infants ( 1 week- 3mths ) born in study period • Term infants > 37 week gestation • Baseline characteristics of infants and mothers available • Exclusions: • those infants with underlying medical conditions • Duplicated blood cultures performed within 3 days and not identifying a new pathogen
Identified all positive blood cultures Samples collected from OPD, ED and in patient setting Positive blood cultures classified as “likely contaminant” and “potential pathogen” Excluding all blood cutlures from infants with underlying medical conditions Excluded duplicates results from within 3 days of positive result Urine and CSF analysis included if performed within 2 days of blood culture acquisition (only positive results) Event Title If Required (Change Text in Footer)
Outcomes • Common pathogens in study period attributing to infant infection with a positive blood culture • E.Coli, GBS and Staph Aureus • Overall Incidence of bacteraemia in infants ( 92/160,818 or 0.57 per 1000 full term births) • E. Coli sepsis – more evenly spread incidence through 3 mhs • GBS – greater incidence initially • Incidence rates compared by age, sex, race
Outcomes Continued No cases of Listeria or Neisseria recorded Only infants with E.Coli, GBS or Strep Pneum bacteraemia had concomitant meningitis Event Title If Required (Change Text in Footer)
Are the results of the study valid? • Did the study address a clearly focused issue? Yes Cleary defined population Outcomes clear • Did the authors use an appropriate method to answer their question? Yes Cohort study was an appropriate study
Detailed Questions • Was the cohort recruited in an acceptable way? Yes • Was the exposure accurately measured to minimise bias? Yes
Detailed questions continued • Was the outcome accurately measured to minimise bias? Can’t Tell Objective measurement (+/-) Excluded some positive blood cultures ( ie. CONS) which may affected end result • A. Have the authors identified all important confounding factors? Yes • B. Have they taken account of the confounding factors in the design and/or analysis? Yes Comorbidity and illness severity considered, age/gender/time of presentation not found to influence outcome
Detailed questions continued • A. Was the follow up of subjects complete enough? Unclear • B. Was the follow up of subjects long enough? Unclear To answer their outcomes follow-up adequate Longer term morbidity not considered- especially those with bacteraemia, UTI and meningitis
8. What are the results of the study? E.Coli bacteraemia > GBS in this study Infants with E.Coli bacteraemia had higher WCC than controls 9. How precise are the results? IQR provided Overall incidence clearly provided Generally precise Event Title If Required (Change Text in Footer)
Results questions 10. Do you believe the results? Yes 11. Can the results be applied locally? Yes Very similar population to that of study 12. Do the results of the study fit with other available evidence? Yes
Will the results help us at SCH? What are the implications for further practice? • Given the low incidence of bacteraemiain this study, is it possible that we use observation as a tool before we do a full septic workup for infants <3mths • Do we need to be more proactive with identifying E.Coli as we are with GBS?
Summary and Conclusions GBS isn’t the only organism worth considering when seeing infants < 3 mths with possible infection Overall incidence of bacteraemia in this study is low.