Download
1 / 44
450 likes | 671 Views
Brucellosis. M.Karimi. Etiology. Brucella: Abortus(Cattle),Melitensis (Sheep,Goat)Suis(Swin),Canis(Dog) G- Coccobacil Aerobic, Non-spore forming Non motile Blood or Choclate agar. Epidemiology. Unpasteurized milk Occupational events. Inoculation in skin ,Eye

E N D
Brucellosis M.Karimi
Etiology • Brucella: Abortus(Cattle),Melitensis (Sheep,Goat)Suis(Swin),Canis(Dog) • G- Coccobacil • Aerobic, Non-spore forming • Non motile • Blood or Choclate agar
Epidemiology • Unpasteurized milk • Occupational events
Inoculation in skin ,Eye (Through abrasion or conjunctiva) Inhalation (Infected aerosol) Ingestion (Meat, Dairy products) Risk of infection depends Nutritional status Immune status Rout of inoculum Species of brucella Pathogenesis
Pathogenesis • Survive& Replicate within phagocytes&Monocytes • Infected macrophages localized within reticuloendothelial system(Granuloma formation in spleen,liver,bone marrow)
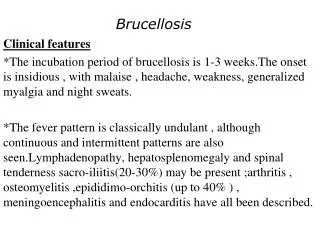
+ History of animal or food exposure Acute or insidious symptoms(2-4 wk after inoculation) Refusal to eat Refusal to bear weight Lassitude FTT Headache Inattention/Depression Abdominal pain Headache Diarrhea Rash Night sweets Weakness Fatigue Cough Vomiting Pharyngitis Clinical manifestationTriad: Fever, Arthralgia/Arthritis,Hepatosplenomegaly
Fever • Hepatosplenomegally • Arthralgia/Arthritis Sacroiliac,Hip,Ankle,
Diagnosis • WBC Normal or low • + History of animal or food exposure • Recovering organisms (blood’ bone marrow’..) • Serum agglutination test: >1/160 (Antibody against Abortus ,Melitensis, Suis, but not Canis) • 2ME
Differential diagnosis • Car-Scratch disease • Typhoid fever • TB • Fungal infections
> or = 9 years old 1- Doxycycline 200 mg/D PO 6 WK + Streptomycin 1 g/D IM 1-2 WK OR Gentamycin 3-5 mg/kg/d IM/IV 1-2 WK -------------------------------------------------- 2- Doxycycline 200 mg/D PO 6 WK + Rifampin 600-900 mg/D PO 6 WK < 9 years old TMP-SMZ: po 45 days (TMP 10 mg/Kg/D) (SMZ 50 mg/KG/D) + Rifampin 15-20 mg/kg/D PO 45 days Treatment
Salmonellae Infections M.Karimi
Etiology Salmonellae (G- ‘Facultative’Bacilli) • Antigens: Flagellum(H)’ Cell wall(O)’ Envelope(Vi) • Serogroups on the basis of O antigen: A’ B’ C1’ C2’ D’ E • Serotypes: S.Typhi’ S.Paratyphi’…. • Transmission: Water’ Food(beef’poultry’milk’egg’..)
Salmonella Gastroentritis (Nontyphoidal) Epidemiology • Age: <4 y/o (< 1y/o) • Source of infection: Poultry’eggs’ egg product ’meats’ • Transmission: Carrier (Human) • Incubation period: 6-72 hr. (usually less than 24 hr.) • Peak incidence: Late summer &Early fall
Pathogenesis • Ingestion • Attached to “M” cells • Phagocytosed by macrophages • Replication • Bacteremia
Clinical manifestations • Self limited diseases: 3-7 days • Onset: Abrupt • Nausea’ Vomiting’ Crampy abdominal pain • Loose watery stool • Malaise’ headache’ chills • Fever 38-38.9 c (70%) for 48 hour
Complications • Dehydration’Shock • Localized infection: Pneumonia Empyema Abscesses Osteomyelitis Septic arthritis Postinfectious arthritis Pyelonephritis meningitis
Diagnosis • Cultures (Stool’ Blood’ Urine’ Bone marrow’ CSF’…)
Treatment • Correction of shock’ dehydration’… • Antibiotics: 1-Infants < 3 mo. 2-Child with immunodeficiency’ Malnutrition Malignancy’ Intravascular catheter or other foreign material
Treatment • Ceftriaxone or Cefotaxime Septicemia’ Enteric fever’ Metastatic site of infection • Amoxicillin • Co-trimaxozole • Fluroqinolones • Chloramphenicol
Clinical manifestation • Infant: mild GE to severe septicemia without diarrhea Fever’ hepatomegaly ’ jaundice’ anorexia’ lethargy’ weight loss • Child: High fever’ malaise ’lethargy’ myalgia’ headache’ rash’ Hepatomegaly’ abdominal pain and tenderness’ diarrhea(50%)’ constipation obtunded ’delirium’ confusion ’splenomegaly’ Macular (Rose spot) or Maculopapolar rash(30%) High T with low PR (Typically each 1 degree above 38.3° C Rise PR 10/min)
Intestinal perforation(0.5-3%) Severe GI hemorrhage(1-10%) Toxic encephalopathy Cerebral thrombosis Acute cerebral ataxia Aphasia Optic neuritis Deafness Transverse myelitis Acute cholecystitis Pneumonia Pyelonephritic Endocarditis Meningitis Osteomyelitis Septic arthritis Complications
Diagnosis Cultures: Blood’ Urine’ Stool’ Bone marrow’ Lymph nodes’ Deudenal fluied’ Reticuloendothelial tissue’ Differential diagnosis Bronchitis Bronchopneumonia Gastroenteritis Influenza Diagnosis & Differential diagnosis
Drugs: Ceftriaxone Ampicillin Chloramphenicol Co-Trimoxozole Ciprofloxacin Azithromycin Surgery Cholecystectomy Treatment
Prognosis • With treatment : Mortality <1% • Without treatment : Relapse up to 10% • Chronic carrier: Excrete S.typhi for more than 3 mo.
Diphtheria • Diphtheria is an acute toxic infection caused by Corynebacterium species, typically Corynebacterium diphtheriae .
Corynebacteria Aerobic, nonencapsulated, non-spore- forming, mostly nonmotile, pleomorphic, gram-positive bacilli
EPIDEMIOLOGY • Spread: • airborne respiratory droplets • direct contact • Asymptomatic respiratory tract carriage is important in transmission. • Skin infection and skin carriage • contaminated milk • infected food handler
Clinical manifestation • Paralysis of the palate and hypopharynx is an early local effect of diphtheritic toxin. • Toxin absorption can lead to systemic manifestations: kidney tubule necrosis, thrombocytopenia, cardiomyopathy, and/or demyelination of nerves
serosanguineous, purulent, erosive rhinitis • Shallow ulceration of the external nares and upper lip • sore throat, fever,Dysphagia,Hoarseness • Malaise,Headache,unilateral or bilateral tonsillar membrane formation • enlarged lymph nodes can cause a bull-neck appearance
DIAGNOSIS: culture • COMPLICATIONS: Toxic Cardiomyopathy Toxic Neuropathy • TREATMENT: Antitoxin penicillins, erythromycin
Tetanus • acute, spastic paralytic illness • Clostridium tetani :motile, gram-positive, spore-forming obligate anaerobe • Neurotoxin
EPIDEMIOLOGY • The most common form, neonatal (or umbilical) tetanus • maternal tetanus :postpartum, postabortal, or postsurgical wound infection • traumatic injury • contaminated suture • intramuscular injection • animal bites • abscesses (including dental abscesses) • chronic skin ulceration • Burns • compound fractures, • frostbite, gangrene, intestinal surgery
CLINICAL MANIFESTATIONS • trismus • generalized tetanus • sardonic smile of tetanus (risus sardonicus)
CLINICAL MANIFESTATIONS • painful spasms of the muscles adjacent to the wound site • Cephalic tetanus : retracted eyelids, deviated gaze, trismus, risus sardonicus, and spastic paralysis of the tongue and pharyngeal musculature
DIAGNOSIS • clinically unimmunized patient (and/or mother) who was injured or born within the preceding 2 wk, who presents with trismus, other rigid muscles • Routine laboratory studies are usually normal
TREATMENT • Surgical wound excision and debridement • human tetanus immunoglobulin (TIG) • Penicillin G • muscle relaxants(Diazepam)
† For children <7 yr of age, DTaP is preferred to tetanus toxoid alone if <3 doses of DTaP have been previously given. If per-tussis vaccine is contraindicated, DT is given. For persons ≥7 yr of age, Td (or Tdap for adolescents 11–18 yr of age) is preferred to tetanus toxoid alone. Tdap is preferred to Td for adolescents 11–18 yr of age who have never received Tdap. Td is preferred to tetanus toxoid for adolescents who received Tdap previously or when Tdap is not available.‡ TIG should be administered for tetanus-prone wounds in HIV-infected patients regardless of the history of tetanus immunizations. § Yes, if ≥10 yr since the last tetanus toxoid-containing vaccine dose.‖ Yes, if ≥5 yr since the last tetanus toxoid-containing vaccine dose CLEAN, MINOR WOUNDS OTHER WOUNDS[*]