Download
1 / 185
1.85k likes | 1.87k Views
RIPBIS Tertiary Supports in SWPBIS Conjoint Behavioral Consultation (CBC) [Collaborative Problem Solving Teams]. John Eagle, Ph.D., & Shannon Dowd-Eagle, Ph.D. SWPBS Subsystems. School-wide. Classroom. Family. Non-classroom. Student. School-wide.

E N D
RIPBISTertiary Supports in SWPBISConjoint Behavioral Consultation (CBC)[Collaborative Problem Solving Teams] John Eagle, Ph.D., & Shannon Dowd-Eagle, Ph.D. Paul V. Sherlock Center on Disabilities @ Rhode Island College, 2009
SWPBS Subsystems School-wide Classroom Family Non-classroom Student Paul V. Sherlock Center on Disabilities @ Rhode Island College, 2009
School-wide 1. Common purpose & approach to discipline 2. Clear set of positive expectations & behaviors 3. Procedures for teaching expected behavior 4. Continuum of procedures for encouraging expected behavior 5. Continuum of procedures for discouraging inappropriate behavior 6. Procedures for on-going monitoring & evaluation Paul V. Sherlock Center on Disabilities @ Rhode Island College, 2009
Non-classroom • Positiveexpectations & routines taught & encouraged • Active supervision by all staff • Scan, move, interact • Precorrections & reminders • Positive reinforcement Paul V. Sherlock Center on Disabilities @ Rhode Island College, 2009
Classroom Classroom-wide positive expectationstaught & encouraged Teaching classroom routines & cues taught & encouraged Ratio of 6-8 positive to 1 negativeadult-student interaction Active supervision Redirections for minor, infrequent behavior errors Frequent precorrectionsfor chronic errors Effective academic instruction & curriculum Paul V. Sherlock Center on Disabilities @ Rhode Island College, 2009
Individual Student Behavioral competence at school & district levels Function-based behavior support planning Team- & data-baseddecision making Comprehensive person-centered planning & wraparound processes Targeted socialskills& self-management instruction Individualized instructional & curricularaccommodations Paul V. Sherlock Center on Disabilities @ Rhode Island College, 2009
Family Continuum of positive behavior support for all families Frequent, regular positive contacts,communications, & acknowledgements Formal & active participation& involvement as equal partner Access to system of integrated school & community resources Paul V. Sherlock Center on Disabilities @ Rhode Island College, 2009
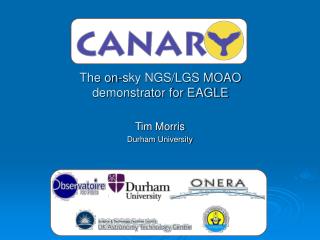
Positive Behavior Interventions & Supports:A Response to Intervention (RtI) Model Tier 1/Universal School-Wide Assessment School-Wide Prevention Systems ODRs, Attendance, Tardies, Grades, DIBELS, etc. Tier 2/Secondary Tier 3/ Tertiary Brief FBA Check-in/ Check-out (CICO) Behavior Education Plan (BEP) Intervention Assessment Daily Progress Report (DPR)(Behavior and Academic Goals) Instructional Groups Social/Problem-solving/ Academic Group Intervention with Individualized Feature (e.g., Check and Connect and Mentoring) Competing Behavior Pathway, Functional Assessment Interview, Scatter Plots, Behavioral Observations, etc. Collaborative Problem Solving Teams Conjoint Behavioral Consultation Teams SIMEO Tools: HSC-T, RD-T, EI-T Wraparound Adapted fromIllinois PBIS Network, 2009 and T. Scott, 2004 Paul V. Sherlock Center on Disabilities @ Rhode Island College, 2009
Paul V. Sherlock Center on Disabilities @ Rhode Island College, 2009
Systems-Response Tool Paul V. Sherlock Center on Disabilities @ Rhode Island College, 2009
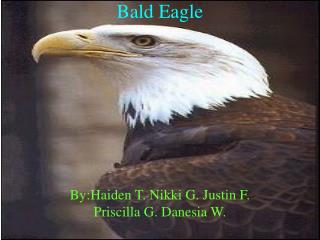
3-Tiered System of Support Necessary Conversations (Teams) UniversalTeam Secondary Systems Team Problem Solving Team Tertiary Systems Team Uses Process data; determines overall intervention effectiveness Uses Process data; determines overall intervention effectiveness Plans SW & Class-wide supports Standing team; uses FBA/BIP process for one youth at a time CICO Universal Support Brief FBA/BIP SAIG Complex FBA/BIP WRAP Group w. individual feature Brief FBA/BIP Paul V. Sherlock Center on Disabilities @ Rhode Island College, 2009 Source: Illinois PPBIS Network
Tier 2/Tier 3 InterventionsTracking Tool:NON-Examples ofData-based Decision-rules for Defining Response Responding to CICO: kid carries that DPR card 2. Responding to Social/Academic instructional groups: kidshows up for group - even if he’s not supposed to be there 3. Responding to Individualized CICO, Groups & Mentoring (i.e. CNC): roughly, maybe about 30-50% of the numbers are circled on the paper sheet (double digits are always good) 4. Responding to Brief Function-Based Interventions: kid says “now he gets why he does what he does and promises never to do that behavior again” 5. Responding to Complex Function-Based Interventions: kid says “now he really gets why he does what he does and promises never to do that behavior again” 6. Responding to Wraparound Plans: kid comes to school every day with a smile, and the kid’s teacher has taken to wearing her original “Woodstock Nation” t-shirt on school spirit days – she’s a happy camper. Paul V. Sherlock Center on Disabilities @ Rhode Island College, 2009 Source: Lucille Eber, Illinois PPBIS Network
Tier 2/Tier 3 InterventionsTracking Tool:Examples ofData-based Decision-rules for Defining Response Responding to CICO: Youth earned a total of 80% of DPR points averaged per day/week for 4 weeks. Responding to Social/Academic Instructional groups: Youth earned a total of 80% of DPR points averaged per day/week for 4 weeks (demonstrating target skill(s) in classroom setting) and has had no new ODRs. Responding to Individualized CICO, Groups & Mentoring (i.e. CNC): Youth earned a total of 80% of DPR points averaged per day/week for 4 weeks, has had no ODRs or ISSs and has improved attendance. 4. Responding to Brief Function-Based Interventions: Over a 4 week period, youth has demonstrated trends of decreased tardies and increased work completion (as demonstrated on individualized DPR). Responding to Complex Function-based Interventions: Youth earned a total of 80% of DPR points averaged per day/week for 4 weeks (demonstrating target skill(s) in classroom setting), 50% reduction in ODRs and improvement in SIMEO. 6. Responding to Wraparound Plans: Improvement in reading skills as measured by DIBELS; and improvement with peer interactions (participating in extracurricular activities and socializing with peers on a regular basis) as measured by SIMEO. Paul V. Sherlock Center on Disabilities @ Rhode Island College, 2009 Source: Lucille Eber, Illinois PPBIS Network
Deciding Which Tertiary Level Intervention is Most Appropriate Complex FBA/BIP (T200): Brief FBA/BIP was not successful AND NONE of Wraparound criteria are present Wraparound (T300+): Youth with multiple needs across home, school, community & life domains Youth at-risk for change of placement The adults in youth’s life are not effectively engaged in comprehensive planning (i.e. adults not getting along well) Paul V. Sherlock Center on Disabilities @ Rhode Island College, 2009 Source: Lucille Eber, Illinois PPBIS Network
Paul V. Sherlock Center on Disabilities @ Rhode Island College, 2009
Benefits of Family Involvement Students • Higher grades, test scores, and graduation rates • Better school attendance • Increased motivation, better self-esteem • Lower rates of suspension • Decreased use of drugs and alcohol • Fewer instances of violent behavior • Greater enrollment in postsecondary education Teachers • Greater morale (and self-esteem) • Teaching effectiveness (proficiency) increases • Job satisfaction goes up • Communication/relations with students, parents, families, and communities improves • Community support of schools increases Parents • Communication/relations with children and teachers improves • Self-esteem goes up • Education level/skills increase • Decision-making skills become stronger • Attitude toward school and school personnel improves Standards for Parent/Family Involvement Programs http://www.pta.org/archive_article_details_1118251710359.html Paul V. Sherlock Center on Disabilities @ Rhode Island College, 2009
Family Involvement in SWPBIS Begins at the Universal Level Paul V. Sherlock Center on Disabilities @ Rhode Island College, 2009
Family Involvement Programs within School-Wide Systems • Intensive, Individual Interventions • Conjoint Behavioral Consultation (CBC) • School-Based Teaming • Wraparound Services • Community Schools • Targeted Group Interventions • Check and Connect • Cross-Setting Social Skills Instruction • Home-School Notes • BEP/BEP-Home • Parent Management Training • Incredible Years Programs • Parent Child Interaction Therapy • Universal Interventions • Four A’s (Christenson & Sheridan) • Epstein’s Six Types of Parent Involvement • AWARE Parenting Program • Systematic Training for Effective Parenting • Positive Discipline Program • Incredible Years Self-Administered Program • Parent Teacher Conferences • Newsletters /Parent Libraries Social-Emotional / Behavioral Systems 1-5% 5-10% 80-90% Paul V. Sherlock Center on Disabilities @ Rhode Island College, 2009
How Do You Involve Families within SWPBIS? Paul V. Sherlock Center on Disabilities @ Rhode Island College, 2009
Family Involvement Programs within School-Wide Systems Paul V. Sherlock Center on Disabilities @ Rhode Island College, 2009
Collaborative Problem Solving Teams within a 3-Tiered Model Paul V. Sherlock Center on Disabilities @ Rhode Island College, 2009
PST in RTI (Burns et al., 2008) Tier 1: look at screening data (ODR, attendance, CBM, AIMSWeb) and identify at-risk students All students are assessed 3-4 times/year Efficient – 5 minutes for assessment Serve in decision making for curriculum and focus on a match between student needs and instruction Review behavior policies and practices Paul V. Sherlock Center on Disabilities @ Rhode Island College, 2009
PST in RTI (Burns et al, 2008) Tier 2 Examine data & identify appropriate interventions for 10-15% of students who are not being successful in Tier 1 Monthly progress monitoring Help determine need for more intense interventions Help determine when student is ready to exit to a less intense intervention Possible Tier II Interventions Supplemental Instruction (Reading Recovery) Peer Tutoring (Duvall, Delquadri, Elliot, & Hall, 1992; Hook & DuPaul, 1999). Behavior Education Program (BEP) (Crone, Horner & Hawkin, 2004) Incredible Years (Webster-Stratton, 2009) Paul V. Sherlock Center on Disabilities @ Rhode Island College, 2009
PST in RTI (Burns et al., 2008) Tier 3: Identify individual interventions Data collected at this level plays a key role in eligibility decisions Paul V. Sherlock Center on Disabilities @ Rhode Island College, 2009
Tier 3: Tertiary Interventions Level 3, tertiary interventions, targets the 1-5% of young children who display persistent challengingsymptoms or behaviors The goal of tertiary interventions is to reduce the frequency, intensity and complexity of a child's maladaptive behavior patterns and provide him/her with suitable, efficient and effective replacement behaviors that will compete with his/her more maladaptive ones. Tertiary interventions are individualized, assessment-based and designed to meet individual needs. Wraparound Paul V. Sherlock Center on Disabilities @ Rhode Island College, 2009
Tier 3: Tertiary Interventions Function-based interventions are developed through the process of functional assessment (FA) and behavior support plans (BSP). Functional assessment determines why the student exhibits challenging behavior. BSPs are most effective when developed by a team with family involvement. Collaborative Problem Solving Teams (Conjoint Behavioral Consultation; CBC) Wraparound Individualized Strategies Sources: Blair, Umbreit, & Eck, 2000; Dunlap & Fox, 1999; Galensky, Miltenberger, Stricker, & Garlinghouse, 2001; Moes & Frea, 2000; Reeve & Carr, 2000). Paul V. Sherlock Center on Disabilities @ Rhode Island College, 2009
Conjoint Behavioral Consultation (CBC; Sheridan & Kratochwill, 1992) CBC is a data-based problem-solving model that systematically joins parents and teachers in the provision of services for children with academic, behavioral, and social concerns. Paul V. Sherlock Center on Disabilities @ Rhode Island College, 2009
Direct Service Model Therapist Child Paul V. Sherlock Center on Disabilities @ Rhode Island College, 2009
Indirect Service Model Consultee (Teacher or Parent) Facilitator / Consultant Child Paul V. Sherlock Center on Disabilities @ Rhode Island College, 2009
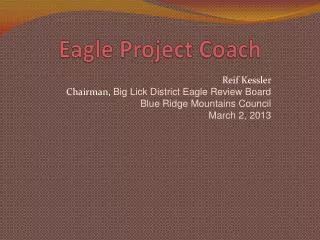
Conjoint Indirect Service Model Consultee (Parent) Facilitator / Consultant Child Consultee (Teacher) Paul V. Sherlock Center on Disabilities @ Rhode Island College, 2009
Conceptual Bases of CBC • Ecological Systems Theory(Bronfrenbrenner, 1979) • Views children in context • Emphasizes reciprocal interactions • Linkages are critical in development of programs • Expanded assessment and intervention contexts • Behavioral Consultation (Bergan & Kratochwill, 1990) • Structured problem solving process • Problem Identification • Problem Analysis • Treatment Implementation • Treatment Evaluation Paul V. Sherlock Center on Disabilities @ Rhode Island College, 2009
Goals of CBC • Outcome: • Improve academic/social/behavioral functioning • Enhanced generalization • Improve skills/knowledge of all parties • Process/Relational: • Increase communication • Foster home-school partnership • Promote greater conceptualization of concern • Promote shared ownership Paul V. Sherlock Center on Disabilities @ Rhode Island College, 2009
CBC – 4 Stage Problem-Solving Process • Needs (Problem) Identification • Needs (Problem) Analysis • Treatment Implementation • Treatment Evaluation • Although the model follows a stagewise progression, it is generally fluid and cyclical in practice. Paul V. Sherlock Center on Disabilities @ Rhode Island College, 2009
Problem Solving Process Needs (Problem) Identification Defining Problem/Directly Measuring Behavior Needs (Problem) Analysis Validating Problem Identify Variables that Contribute to Problem Functional Assessment Development Plan Treatment Evaluation Was it Effective? Follow-up Procedures Generalization / Maintenance Treatment Implementation Implement with Fidelity Progress Monitor Treatment Modifications Paul V. Sherlock Center on Disabilities @ Rhode Island College, 2009
Needs Identification Traditional Collaborative • Schedule meeting • Team Membership • Invite key personnel and family members • Prioritize and define needs • Determine discrepancy between current and expected level of performance • Establish data collection procedure • Schedule meeting • Convenient time • Escort to meeting • Room arrangement • Team Membership • Include only necessary staff • Ask family who to include • Prioritize and define needs • Identify strengths (all settings) • Frame needs in positive language • Determine discrepancy between current and expected level of performance • Avoid problem glorification • Establish data collection procedure • Suggest EASY strategies Paul V. Sherlock Center on Disabilities @ Rhode Island College, 2009
Needs Analysis Traditional Collaborative • Evaluate baseline data • Set Goal • Where is the instructional mismatch • Conduct FBA • Develop plan • Re-affirm data collection • Evaluate baseline data • Check in with staff/family between meetings • Praise data collection efforts • Set Goal • Determine instructional mismatch • Use unifying language (“our,” “we”) • Conduct FBA • Gather information from both home and school settings • Point out similarities across settings • Highlight team members’ expertise & knowledge of child • Develop plan • Identify plan components across setting • Buy in and social validity • Re-affirm data collection procedures Paul V. Sherlock Center on Disabilities @ Rhode Island College, 2009
Needs Analysis • Goal Setting • Set a realistic short term goal • Cross-setting FBA • Parents and teachers KNOW the student and how he/she functions in home and school setting • Can provide a cultural context • Cross-setting plan development • What motivates the child? • Is the plan feasible (resources, time)? The best plan will not be implemented if the team members are unwilling or unable to implement it Paul V. Sherlock Center on Disabilities @ Rhode Island College, 2009
Plan Implementation Traditional Collaborative • Measure Treatment Integrity • Monitor plan implementation • Plan modifications • Measure Treatment Integrity • Provide written information • Checklist to self-monitor • Monitor plan implementation and provide support/training • Does team member know what to do? • Does team member know how to do it? • Does team member believe it will work? • Is there enough time/resources? • Plan modifications Paul V. Sherlock Center on Disabilities @ Rhode Island College, 2009
Plan Evaluation Traditional Collaborative • Determine if goals have been met • Compare pre/post data • Discuss next step • Plan modifications • Generalization / maintenance • Referral • Determine if goals have been met • Compare pre/post data • Present graphs showing progress • Reinforce joint efforts • Discuss next step • Plan modifications • Highlight parents/teachers role in decision-making process • Social validity? Plan acceptable? • Highlight skills in addressing future concerns • Generalization/maintenance • Referral Paul V. Sherlock Center on Disabilities @ Rhode Island College, 2009
Plan Evaluation School Home Paul V. Sherlock Center on Disabilities @ Rhode Island College, 2009
A few skills needed for Collaborative PS • Define TB’s in objective terms • Promote social competencies / replacement behaviors • Knowledge of user-friendly data collection strategies • Conduct FBA via interviews, observations, checklists using an ecological perspective • Knowledge of EBI • Link FBA to EBI’s • Determine methods for TX integrity • Evaluation of interventions • Facilitate the problem-solving process with integrity • Elicit meaningful information from tees / interviewing skills • Relationship building & conflict management skills • The ability to foster H-S collaboration via process and content Paul V. Sherlock Center on Disabilities @ Rhode Island College, 2009
Microskills Open Questions Minimal Encouragers Reflecting Self-disclosure Paraphrasing Perspective Taking Pointing out similar experiences among consultees. Listening and acknowledging different perspectives. Using empathy and accurate understanding Conflict management Focus on mutual goals/ interests Use language to unify Reframing Use an agenda to focus on a common theme Read nonverbal language Building relationships Point out participant contributions Develop opportunities for positive communication Accept participants “where there are at” Present a non-deficit approach Collaboration is NOT lip service! Paul V. Sherlock Center on Disabilities @ Rhode Island College, 2009
Problem Solving Process 1. Needs/Problem Identification 2. Needs/Problem Analysis 3. Treatment Plan Implementation 4. Treatment Plan Evaluation Paul V. Sherlock Center on Disabilities @ Rhode Island College, 2009
Paul V. Sherlock Center on Disabilities @ Rhode Island College, 2009
STAGE = INTERVIEW Paul V. Sherlock Center on Disabilities @ Rhode Island College, 2009
CBCStage INeeds IdentificationPremeeting / Meeting 1 Paul V. Sherlock Center on Disabilities @ Rhode Island College, 2009
Needs/Problem Identification Content goals • Identify student strengths and needs • Prioritize, specify, and define target behavior • Conduct a preliminary Functional Behavioral Assessment (FBA) • Establish a baseline data collection procedure Paul V. Sherlock Center on Disabilities @ Rhode Island College, 2009
Oh wait…we are working with people…. Process goals • Establish/improve a working relationship among team • HOW???? • Validate shared goals of supporting the child. • HOW???? • Identify the strengths of the child, family and school. • Increase communication and knowledge regarding the child, goals, concerns, and culture of family and school. • HOW??? Paul V. Sherlock Center on Disabilities @ Rhode Island College, 2009
Identifying Target Needs Consider • Identify a response chain and target the first behavior in the chain • Select behaviors that will likely generalize to other behaviors • Organize behaviors in terms of their topographical or functional properties • Prioritize behaviors that have general utility and that the environment will likely maintain. • Change the “easiest” behavior to encourage further treatment efforts Paul V. Sherlock Center on Disabilities @ Rhode Island College, 2009
Defining Target Needs • Provide a precise description of the target concern • Focus on specific aspects of the behavior that can be understood by an independent observer Criteria for good behavioral definition • Objective: observable characteristics of behavior must be countable and measurable • Clear: unambiguous, specific, and reliable • Complete: the boundaries of what is to be included and excluded should be delineated Paul V. Sherlock Center on Disabilities @ Rhode Island College, 2009