Download
1 / 59
590 likes | 608 Views
Explore the mental health challenges faced by doctors, including stress, burnout, and disorders. Learn about the impact on individuals and the community and the factors contributing to these issues. Discover strategies for improving doctor well-being.

E N D
The Mental Health of the Profession Tony Davis
Scope of the presentation Health status of doctors Work issues confronting clinicians The “stressed” doctor The “disordered” doctor Epidemiology of mental illness Clinician vulnerability
Relatively good physical health • Low prevalence of smoking, CV disease, cancer • Similar risks for most mental health problems • Psychological vulnerabilities predispose to certain mental disorders • Reduced likelihood of early or optimal treatment
Concerns Reported high rates of: • Depression • Alcoholism • Drug dependence • Marital discord • Suicide
Shortage of doctors • Aging workforce • More part-time practitioners • Change in work culture of graduates • Escalating public demands • Financial pressures/decline in income (?) • Loss of status (?) • Loss of autonomy • Explosion of alternative therapists (“complementary medicines”) • Patient complaints
“Work Stress” Sources: • The Consultation • Interpersonal Issues • Organisational Issues • External stressors • Situational factors • Personality factors
The Consultation Inherently complex process (interpersonally and cognitively) Dealing with: • difficult, challenging, dependant or unresponsive patients • suffering, pain, anguish • distressed, traumatised patients • death and dying • uncertainty • confidentiality • view of doctor as “healer” or “saviour”
Interpersonal issues • Long/unsociable working hours • High patient demand (internet age) • Patient mistrust/negativity/hostility • Conflicts with partners, staff and colleagues • Spill-over of work demands and tension into family life
Organisational issues • Lack of resources • Lack of administrative support • Bureaucratic interference/demand for documentation, accountability, compliance • Inflexible/hierarchical career paths • Lack of monetary reward for consultative medicine • Shift in power/control away from doctors
External stressors • Work being constantly assessed by patients and families • High emotional demand and high level of responsibility • Risks of malpractice litigation • Scrutiny by the Health Insurance Commission • Often no clear supervisory structure or mentoring programme
And: • Variable degree of peer support • No formal surveillance of psychological wellbeing • No form of employee assistance programmes • Little regular feedback about success • Increased corporatisation of health care
Situational factors • Marital, relationship, family issues – competing needs of patients and family • Financial pressures • Disruption sleep/wake cycle • Physical illness/limitations
Personality traits/characteristics • Obsessional (perfectionistic, rigid) • Ambitious • Self-sacrificing/need to please • Low tolerance uncertainty/ambiguity • Difficulty with emotional expression • High expectations of self • Struggle with omnipotence • Struggle with ambivalence/patient dependency
Personality traits/characteristics • Some traits adaptive for work practice • Can contribute to vulnerability for mental health problems
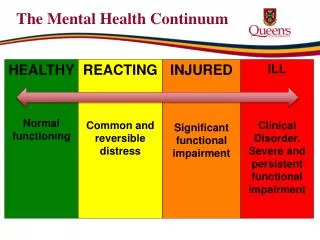
Spectrum of Disorder • “Impaired” – small proportion, mental illness or substance abuse • “Troubled” – larger group, effected by stress (at risk of becoming impaired?) • “Dissatisfied” – complain about “system” and its demands, contemplate leaving the profession (at risk of “burn out”?)
“Burnout”/”Compassion fatigue” • Physical and mental exhaustion • Negative self-concept • Negative job attitude • Loss of concern and feeling for patients
“Burnout”/”Compassion fatigue” Results in: • Loss of empathy • Intolerance of patients’ demands • Irritability, impatience
Outcomes / Effects of “Burnout” For the doctor Reduced quality of life Increased risk of physical, mental health problems: • Depression • Alcoholism • Drug abuse • Suicide
For the community Dysfunctional practitioner – poor work quality, errors and mistakes Depletion rare resources through early retirement or departure from medical practice Outcomes / Effects of “Burnout”
Epidemiology of Mental Illness • Few epidemiological studies (Australia) • Small numbers, uncontrolled studies • Selection bias • Retrospective designs • Rating scales of questionable validity • Many studies not comparable in sample and diagnostic criteria
Epidemiology of Mental Illness • Most study doctors treated for illness • Many doctors don’t seek formal treatment • Informal treatment not documented
Epidemiology of Mental Illness • Large gaps in literature re prevalence of mental disorder in GP’s, private sector specialists and rural/remote doctors • Most studies from UK, Europe and USA • Little comparative data from other professional groups
Beyond Blue Investigated mental health of medical students and doctors Report: “The mental health of doctors. A systematic literature review” (2009) Completed national mental health survey (2010) Developed national doctor’s mental health program
Literature Review Focus on 10 topics: 1 – Prevalence of anxiety and depression 2 – Prevalence of substance abuse and self- medication 3 – Suicide rates 4 – Risk factors for anxiety and depression 5 - Help-seeking rates for anxiety and depression
Literature Review 6 – Barriers to help-seeking for mental health care 7 – Interventions for anxiety and depression 8 – Attitudes of medical colleagues 9 – Impact on patient care 10 – Impact on work and family life
Beyond Blue - Depression Prevalence – 14-60% No higher than other professionals Higher in male practitioners than general population (?)
Beyond Blue - Anxiety Prevalence 18-55% Weak evidence – higher than general population No different to other professionals
Beyond Blue - Substance Abuse No evidence more alcohol abuse than general population and other professionals Less common (?) Drug use similar to general population and other professionals
“Suicide rates amongst physicians” Meta-analysis of 33 studies Male – 1.41 higher risk cf gen population Female – 2.27 higher risk Lower overall mortality rates Psychiatrists at highest risk (?) Different to other professional groups (?) Most common – drugs/poisoning (Schernhammer & Colditz, 2004)
Suicide in doctors - psychological autopsy study England and Wales, 1991 - 93 N = 38 (28M, 10F) 44% < 35 years 25 had psychiatric illness, mainly depression (21), alcohol or drug abuse 15 receiving treatment (GP or Specialist) at time of death 9 had previous suicide attempts 74% self-poisoning (Hawton et al, 2001)
Suicide in doctors - psychological autopsy study • 25 had significant work problems • 14 had relationship problems • 10 had financial problems • most had multiple, inter-related problems
Suicide – specialty groups 6 studies 3 studies - highest rate in psychiatrists
National Mental Health Survey (2010) 42,942 doctors 6,658 medical students 27% response rate Kessler 10 (K10) Scale
NMHS - 2010 Very high psychological distress - greater in doctors compared to general population and other professionals (3.4% vs 2.6% vs 0.7%) Particularly in doctors aged less than 30
NMHS - 2010 21% reported ever being diagnosed with, or treated for, depression 6% had current depression similar level to general population, higher than other professionals (6.2% vs 6.2% vs 5.3%) 9% reported diagnosed or treated for anxiety disorder 3.7% had current diagnosis
NMHS - 2010 24.8% had thoughts of suicide prior to the last 12 months (general population 13.3%, other professionals 12.8%) 10.4% had thoughts of suicide in previous 12 months 2% had attempted suicide
“Suicide in medical doctors and nurses” 1990-2007 Queensland suicide register Males: lower rates than education professionals and general population Females: higher rates than education professionals, similar rates to general population (Kolves et al, 2013)
A Comment on "Problem Doctors” (Smith, 1997) “Medical students are put through a gruelling course and exposed much younger then their non-medical friends to pain, sickness, death and the perplexity of the soul. And all of this within an environment where “real doctors” get on with the job and only the weak weep or feel distressed.”
Smith (1997) cont “After qualification, doctors work absurdly hard, are encouraged to tackle horrible problems with inadequate support, and then face a lifetime of pretending that they have more powers than they actually do. And all this within an environment where narcotics are readily available.”
Choice of medical career “Neurotic” factors: • Attempt to resolve conflicts from childhood – related to parental inadequacy, illness, emotional neglect • Attempt to compensate for poor self-esteem • Defence against death anxiety