Download
1 / 1
10 likes | 147 Views
Breast Cancer and Hormone Therapy Student: Lisa Kiesow Faculty: Dr. Nancy Bachman. Abstract

E N D
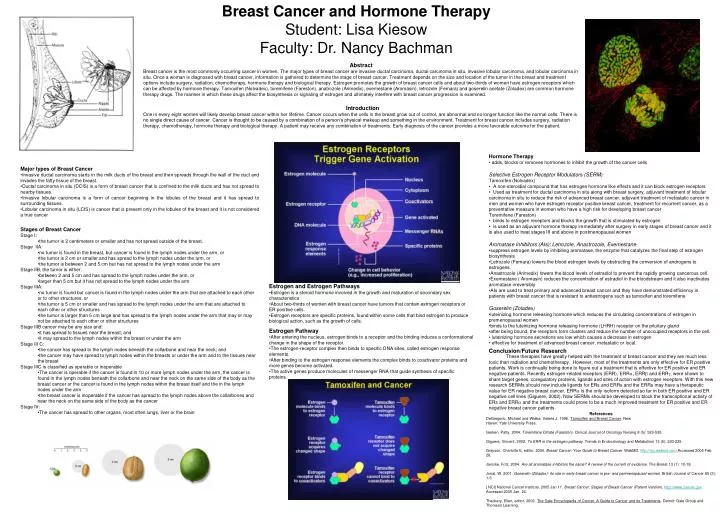
Breast Cancer and Hormone Therapy Student: Lisa Kiesow Faculty: Dr. Nancy Bachman Abstract Breast cancer is the most commonly occurring cancer in women. The major types of breast cancer are invasive ductal carcinoma, ductal carcinoma in situ, invasive lobular carcinoma, and lobular carcinoma in situ. Once a woman is diagnosed with breast cancer, information is gathered to determine the stage of breast cancer. Treatment depends on the size and location of the tumor in the breast and treatment options include surgery, radiation, chemotherapy, hormone therapy and biological therapy. Estrogen promotes the growth of breast cancer cells and about two-thirds of women have estrogen receptors which can be affected by hormone therapy. Tamoxifen (Nolvadex), toremifene (Fareston), anatrozole (Arimedix), exemestane (Aromasin), letrozole (Femara) and goserelin acetate (Zoladex) are common hormone therapy drugs. The manner in which these drugs affect the biosynthesis or signaling of estrogen and ultimately interfere with breast cancer progression is examined. Introduction One in every eight women will likely develop breast cancer within her lifetime. Cancer occurs when the cells in the breast grow out of control, are abnormal and no longer function like the normal cells. There is no single direct cause of cancer. Cancer is thought to be caused by a combination of a person’s physical makeup and something in the environment. Treatment for breast cancer includes surgery, radiation therapy, chemotherapy, hormone therapy and biological therapy. A patient may receive any combination of treatments. Early diagnosis of the cancer provides a more favorable outcome for the patient. • Hormone Therapy • adds, blocks or removes hormones to inhibit the growth of the cancer cells • Selective Estrogen Receptor Modulators (SERM) • Tamoxifen (Nolvadex) • A non-steroidial compound that has estrogen hormone like effects and it can block estrogen receptors • Used as treatment for ductal carcinoma in situ along with breast surgery, adjuvant treatment of lobular carcinoma in situ to reduce the risk of advanced breast cancer, adjuvant treatment of metastatic cancer in men and women who have estrogen receptor positive breast cancer, treatment for recurrent cancer, as a preventative measure in women who have a high risk for developing breast cancer • Toremifene (Fareston) • binds to estrogen receptors and blocks the growth that is stimulated by estrogen • is used as an adjuvant hormone therapy immediately after surgery in early stages of breast cancer and it is also used to treat stages III and above in postmenopausal women • Aromatase Inhibitors (AIs): Letrozole, Anastrozole, Exemestane • suppress estrogen levels by inhibiting aromatase, the enzyme that catalyzes the final step of estrogen biosynthesis • Letrozole (Femara) lowers the blood estrogen levels by obstructing the conversion of androgens to estrogens. • Anastrozole (Arimedix) lowers the blood levels of estradiol to prevent the rapidly growing cancerous cell. • Exemestane ( Aromasin) reduces the concentration of estradiol in the bloodstream and it also inactivates aromatase irreversibly • AIs are used to treat primary and advanced breast cancer and they have demonstrated efficiency in patients with breast cancer that is resistant to antiestrogens such as tamoxifen and toremifene • Goserelin (Zoladex) • luteinizing hormone releasing hormone which reduces the circulating concentrations of estrogen in premenopausal women • binds to the luteinizing hormone releasing hormone (LHRH) receptor on the pituitary gland • after being bound, the receptors form clusters and reduce the number of unoccupied receptors in the cell. • luteinizing hormone secretions are low which causes a decrease in estrogen • effective for treatment of advanced breast cancer, metastatic or local. • Major types of Breast Cancer • Invasive ductal carcinoma starts in the milk ducts of the breast and then spreads through the wall of the duct and invades the fatty tissue of the breast. • Ductal carcinoma in situ (DCIS) is a form of breast cancer that is confined to the milk ducts and has not spread to nearby tissues. • Invasive lobular carcinoma is a form of cancer beginning in the lobules of the breast and it has spread to surrounding tissues. • Lobular carcinoma in situ (LCIS) is cancer that is present only in the lobules of the breast and it is not considered a true cancer • Stages of Breast Cancer • Stage I: • the tumor is 2 centimeters or smaller and has not spread outside of the breast. • Stage IIA: • no tumor is found in the breast, but cancer is found in the lymph nodes under the arm, or • the tumor is 2 cm or smaller and has spread to the lymph nodes under the arm, or • the tumor is between 2 and 5 cm but has not spread to the lymph nodes under the arm • Stage IIB, the tumor is either: • between 2 and 5 cm and has spread to the lymph nodes under the arm, or • larger than 5 cm but it has not spread to the lymph nodes under the arm • Stage IIIA: • no tumor is found but cancer is found in the lymph nodes under the arm that are attached to each other or to other structures, or • the tumor is 5 cm or smaller and has spread to the lymph nodes under the arm that are attached to each other or other structures • the tumor is larger than 5 cm large and has spread to the lymph nodes under the arm that may or may not be attached to each other or other structures • Stage IIIB cancer may be any size and: • it has spread to tissues near the breast; and • it may spread to the lymph nodes within the breast or under the arm • Stage III C: • the cancer has spread to the lymph nodes beneath the collarbone and near the neck; and • the cancer may have spread to lymph nodes within the breasts or under the arm and to the tissues near the breast • Stage IIIC is classified as operable or inoperable • The cancer is operable if the cancer is found in 10 or more lymph nodes under the arm, the cancer is found in the lymph nodes beneath the collarbone and near the neck on the same side of the body as the breast cancer or the cancer is found in the lymph nodes within the breast itself and the in the lymph nodes under the arm • the breast cancer is inoperable if the cancer has spread to the lymph nodes above the collarbones and near the neck on the same side of the body as the cancer • Stage IV: • The cancer has spread to other organs, most often lungs, liver or the brain • Estrogen and Estrogen Pathways • Estrogen is a steroid hormone involved in the growth and maturation of secondary sex characteristics • About two-thirds of women with breast cancer have tumors that contain estrogen receptors or ER positive cells. • Estrogen receptors are specific proteins, found within some cells that bind estrogen to produce biological action, such as the growth of cells. • Estrogen Pathway • After entering the nucleus, estrogen binds to a receptor and the binding induces a conformational change in the shape of the receptor. • The estrogen-receptor complex then binds to specific DNA sites, called estrogen response elements. • After binding to the estrogen response elements the complex binds to coactivator proteins and more genes become activated. • The active genes produce molecules of messenger RNA that guide synthesis of specific proteins. Conclusion/Future Research These therapies have greatly helped with the treatment of breast cancer and they are much less toxic than radiation and chemotherapy. However, most of the treatments are only effective for ER positive patients. Work is continually being done to figure out a treatment that is effective for ER positive and ER negative patients. Recently estrogen-related receptors (ERR), ERR, ERR and ERR, were shown to share target genes, coregulatory proteins, ligands and sites of action with estrogen receptors. With this new research SERMs should now include ligands for ERs and ERRs and the ERRs may have a therapeutic value for ER negative breast cancer. ERR is the only isoform detected so far in both ER positive and ER negative cell lines (Giguere, 2002). Now SERMs should be developed to block the transcriptional activity of ERs and ERR and the treatments could prove to be a much improved treatment for ER positive and ER negative breast cancer patients. References DeGregorio, Michael and Wiebe, Valerie J. 1996. Tamoxifen and Breast Cancer. New Haven: Yale University Press. Gerken, Patty. 2004. Toremifene Citrate (Fareston). Clinical Journal of Oncology Nursing 8 (5): 529-530. Giguere, Vincent. 2002. To ERR in the estrogen pathway. Trends in Endocrinology and Metabolism 13 (5): 220-225. Grayson, Charlotte E, editor. 2004. Breast Cancer: Your Guide to Breast Cancer. WebMD. http://my.webmd.com Accessed 2005 Feb. 28. Janicke, Fritz. 2004. Are all aromatase inhibitors the same? A review of the current of evidence. The Breast 13 (1): 10-18. Jonat, W. 2001. Goserelin (Zoladex)- its role in early breast cancer in pre- and perimenopausal women. British Journal of Cancer 85 (2): 1-5. [ NCI] National Cancer Institute. 2005 Jan 11. Breast Cancer: Stages of Breast Cancer (Patient Version).http://www.cancer.gov. Accessed 2005 Jan. 24. Thackery, Ellen, editor. 2002. The Gale Encyclopedia of Cancer. A Guide to Cancer and its Treatments. Detroit: Gale Group and Thomson Learning.