Download
1 / 1
10 likes | 214 Views
W. Mermershtain , Y. Zalcberg , K.Rouvinov , I.Gusakova , S.Ariad. Department of Oncology, Soroka University Medical Center, and Faculty of Health Science, Ben-Gurion University of the Negev, Beer- Sheva , Israel.

E N D
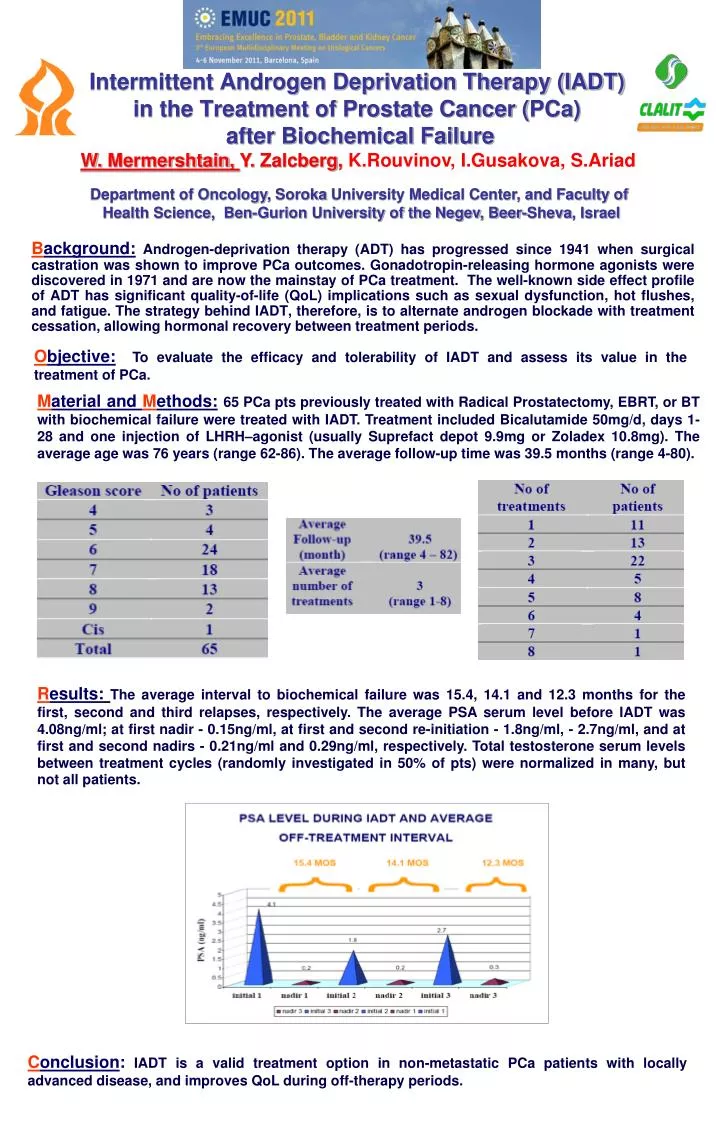
W. Mermershtain, Y. Zalcberg, K.Rouvinov, I.Gusakova, S.Ariad Department of Oncology, Soroka University Medical Center, and Faculty of Health Science, Ben-Gurion University of the Negev, Beer-Sheva, Israel Objective:To evaluate the efficacy and tolerability of IADT and assess its value in the treatment of PCa. Intermittent Androgen Deprivation Therapy (IADT) in the Treatment of Prostate Cancer (PCa) after Biochemical Failure Material and Methods:65 PCa pts previously treated with Radical Prostatectomy, EBRT, or BT with biochemical failure were treated with IADT. Treatment included Bicalutamide 50mg/d, days 1-28 and one injection of LHRH–agonist (usually Suprefact depot 9.9mg or Zoladex 10.8mg). The average age was 76 years (range 62-86). The average follow-up time was 39.5 months (range 4-80). Background:Androgen-deprivation therapy (ADT) has progressed since 1941 when surgical castration was shown to improve PCa outcomes. Gonadotropin-releasing hormone agonists were discovered in 1971 and are now the mainstay of PCa treatment. The well-known side effect profile of ADT has significant quality-of-life (QoL) implications such as sexual dysfunction, hot flushes, and fatigue. The strategy behind IADT, therefore, is to alternate androgen blockade with treatment cessation, allowing hormonal recovery between treatment periods. Results:The average interval to biochemical failure was 15.4, 14.1 and 12.3 months for the first, second and third relapses, respectively. The average PSA serum level before IADT was 4.08ng/ml; at first nadir - 0.15ng/ml, at first and second re-initiation - 1.8ng/ml, - 2.7ng/ml, and at first and second nadirs - 0.21ng/ml and 0.29ng/ml, respectively. Total testosterone serum levels between treatment cycles (randomly investigated in 50% of pts) were normalized in many, but not all patients. Conclusion:IADT is a valid treatment option in non-metastatic PCa patients with locally advanced disease, and improves QoL during off-therapy periods.