Download
1 / 12
120 likes | 257 Views
Summary of Neuropathological and Clinical Features of PDD. Clive Ballard, MD Professor of Age Related Diseases Institute of Psychiatry King’s College London. Overview. PDD is a distinct dementia syndrome PDD can be diagnosed unambiguously in routine clinical practice

E N D
Summary of Neuropathological and Clinical Features of PDD Clive Ballard, MD Professor of Age Related DiseasesInstitute of PsychiatryKing’s College London
Overview • PDD is a distinct dementia syndrome • PDD can be diagnosed unambiguously in routine clinical practice • PDD is a rational target for treatment
Genetic Associations of PDD in Familial PD—Kurz et al, 2006† SN = Sub-stantia nigra; NC = Neocortex. † Kurz et al. Dementia and Geriatr Cog Disorders. In press.
Relationship Between Pathology and Duration of PD Before Dementia † Aarsland D, et al. Ann Neurol. 2005:58;773-776. ‡ Perry R, et al. Neurol. 2006. In press. § Ballard C, et al. Am J Psychiat. 2004:161;843-849.
PDD Predicts a Characteristic Neuropathologic and Clinical Profile • Lewy body pathology (LBP) is the predominant substrate of cognitive decline in PDD • Overlapping AD plaque pathology is not the main correlate of dementia in PDD patients • 93% to 94% of patients with PDD lack sufficient pathologic changes to meet diagnostic criteria for AD • Dementia in PDD has a characteristic profile of neuropsychiatric, cognitive, neurologic, and autonomic features
Attention and Fluctuating Attention in PDD and AD p < 0.0001 p < 0.0001 Ballard C, et al. Neurology. 2002; 59:1714-1720.
Clinical Symptoms of PDD vs AD Ballard C, et al. Am J Psych. 1999;156:1039-1045. Ballard C, et al. J Clin Psych. 2001;2001:46-49.
Autonomic Function (Parasympathetic) in AD and PDD PDD vs. AD: p-value <0.05 for all comparisons. PDD vs. Controls: p-value <0.001 for all comparisons. Kenny RA, et al. Dementia with Lewy Bodies and Parkinson’s Disease Dementia. 2006. Taylor & Francis Pub.
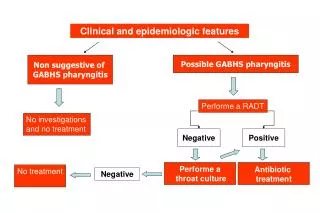
PDD Can be Diagnosed Simply and Unambiguously in Routine Clinical Practice • Diagnosis of PDD is straightforward in routine clinical practice using 3 simple principles • Established diagnosis of Parkinson’s disease • Developing dementia at least 1 to 2 yrs after onset of PD • Exclusion of other causes of dementia, eg, VaD, MSA, PSP
Severe Neuroleptic Sensitivity Reactions in PDD and AD • Severe neuroleptic sensitivity reactions (NSR), characterized by severe parkinsonism, autonomic instability, increased confusion, rhabdomyolysis, and often death • Severe NSR occurs in • > 30% of DLB†‡§ and PDD† • 0% of AD†‡§ † Aarsland D, et al. J Clin Psych. 2005;66:633-637. ‡ McKeith I, et al. BMJ. 1992;305:673-678. § Ballard C, et al. Lancet. 1998;351:1032-1033.
Cholinergic Deficits in PDD • There is established cholinergic deficit in PDD • The cholinergic deficits are associated with many of the key neuropsychiatric symptoms and cognitive deficits † AChE total/AChE 10S form. ‡ Included PD/PDD together.
Conclusions • Lewy body-related alpha-synucleinopathy is the pathology predominantly associated with cognitive impairment in PDD • PDD can most effectively be diagnosed using simple clinical criteria based on the presence of PD and the time course of development of dementia • The shared cholinergic deficit in PDD and AD presents a common treatment target