Download

1 / 56
560 likes | 823 Views
SPUC : Breast lesions. Sharon B. Sams, MD MPH 1/24/2014. 26 year old female Mobile well circumscribed breast mass Non-painful. Case 1: Clinical history . Proliferation of epithelium and stroma Prominent glandular (adenosis-like) proliferation

E N D
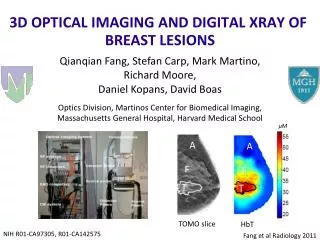
SPUC: Breast lesions Sharon B. Sams, MD MPH 1/24/2014
26 year old female • Mobile well circumscribed breast mass • Non-painful Case 1: Clinical history
Proliferation of epithelium and stroma • Prominent glandular (adenosis-like) proliferation • Well circumscribed lesion with a sharply defined border Case 1: Histopathology
Case 1 Diagnosis:Tubular adenoma Variant of Fibroadenoma
Most common in young women (20-40) • Thought to arise in the TDLU, no elastic tissue • Biphasic tumors with concurrent proliferation of stroma and glandular components • “Adult” FA: 90%; Juvenile FA:10% • Two basic microscopic patterns of adult FA • Intracanalicular: ducts compressed by stroma into elongated linear structures with slit like lumen • Pericanalicular: ducts not compressed Fibroadenoma (FA)
Characteristic of the stroma vary from one FA to another but tend to be homogenous in a single lesion • Proportion of stroma to glands are evenly balanced throughout lesion • Mitotic figures rare in FA • Elastic tissue is absent • Borders well circumscribed Fibroadenoma (FA) vs. Phyllodes tumors
Complex FA: has been used to describe FAs with cysts > 3mm, sclerosing adenosis, epithelial calcifications or papillary apocrine change • Dupont, Page, Parl et al. (1994): reported increased subsequent risk of breast cancer • Sklair-Levy et al. (2008): Complex FA are: • Smaller, older patients • Low incidence of associated malignancy “Complex FA”
13 year old female • Single large painless rapidly growing mass Case 2: Clinical history
Well circumscribed lesion with a sharply defined border • Proliferation of epithelium and stroma • Moderately cellular stroma • No significant stromal atypia or mitotic activity • Epithelial hyperplasia without atypia Case 2: Histopathology
Case 2 Diagnosis: Juvenile (Giant) fibroadenoma Another “variant” of Fibroadenoma
Grossly indistinguishable from adult FA • Clinical: • Young age (less than 20 years) • Recent rapid growth • Microscopic: • Stromal cellularity typically condensed around epithelial structures • Often pericanalicular pattern • Epithelial hyperplasia with mild cytologic pleomorphism, atypia and mitotic figures • Well circumscribed border “Juvenile” FA
72 year old female • Large palpable painless mass with recent rapid enlargement Case 3: Clinical History
Poorly differentiated malignancy • Extensive necrosis • Sarcomatous differentiation including markedly pleomorphic cells, osteoclastic giant cells and osteoid deposition • No distinct glandular component Case 3: Histopathology
Differential diagnosis: • High grade phyllodes tumors • Sarcomas • Metaplastic carcinoma Case 3: Differential Diagnosis
Strong positive expression for Vimentin and CD10 in tumor cells • Rare positive expression for panCK, CK 5/6 and p63 in tumor cells Case 3: IHC result
Clinical: • ~1% of breast cancers • Age range is similar to other types of breast carcinoma • The tumors seem to grow faster then other types • No specific mammographic features, although may have a circumscribed contours • Gross Pathology: • Mean size 4 cm which is larger than ductal carcinoma • Typically firm and nodular • May have cystic denegation (typically in squamous metaplasia) Metaplastic carcinoma
Morphologically heterogenous group traditionally divided into two categories: • Squamous metaplasia • Heterologous (pseudosarcomatous) metaplasia • Bone, cartilage, and/or undifferentiated round or spindle cells • However this is arbitrary as many tumors exhibit both types of growth Metaplastic carcinoma
High grade metaplastic carcinomas • High grade adenocarcinoma AND dominant areas of spindled/sarcomatoid, squamous • Low grade metaplastic carcinomas (rare) • Low grade adenosquamous • Typically smaller with ill-defined borders • Better prognosis, metastasis rare • Low grade spindle cell carcinoma Metaplastic carcinoma
Immunohistochemical studies are useful for spindle cell tumors lacking a distinct epithelial component • Cytokeratins: Pancytokeratin, Cam5.2 CK5/6 CK7 MA903 • Myoepitheilal markers p63 (preferred), CD10, SMA • Majority are “triple negative” for ER, PR and Her2 Metaplastic carcinoma
34 year old female • Prior history of malignancy in contralateral breast Case 4: Clinical History
Anastomosing vascular channels • Hyperchromatic pleomorphic endothelial cells • Areas of necrosis and hemorrhage (“blood lakes”) • Rare nodules composed of spindle cells with few vascular spaces Case 4: Histopathology
Angiosarcoma arises in the breast more often than in any other organ • It is the most common primary breast sarcoma • Clinical • Painless mass, may have blue/purple discoloration of skin • May develop asynchronous primary or metastatic contralateral angiosarcoma Angiosarcoma
Angiosarcoma Picture from: Ann Surg Oncol. 2012 August; 19(8): 2700–2706. Published online 2012 March 31. doi: 10.1245/s10434-012-2310-x
These can arise: • Spontaneously • Mean age 34 • Following radiation therapy for prior breast cancer • Typically >50 when treated for breast cancer, mean age of angiosarcoma 69 years • Post radiation interval ranges from 3-10 years with majority occurring within 6 years • Interval to diagnosis of angiosarcoma inversely related to age, decreasing with advancing age • In the setting of chronic edema (Stewart-Treves syndrome) • Pathogenesis unknown • Average interval between mastectomy (cause of edema) and development of angiosarcoma: 10 years • Most common location: upper inner or medial arm Angiosarcoma
Differential diagnosis: • Benign vascular lesions (angiolipoma, hemangioma • Atypical vascular lesions (AVL) • Possibly angiosarcoma precursor however majority have benign behavior • Other sarcomas, melanoma, poorly differentiated carcinoma, malignant phyllodes tumor • Immunohistochemical studies: • Variable expression of vascular markers, particularly radiation associated AS (D2-40, CD31, CD34, ) • Typically CK negative Angiosarcoma
Prognosis: • Donell et al. (1981): Morphologically heterogenous group in which grade is prognostically significant (n=40) • Nascimento et al. (2009): clinicopathologic analysis suggesting that grade is not prognostic (n=49). *** however data lumps intermediate and high grade • Correlation between age of diagnosis and tumor grade (Rosen et al. 1988) • Median age with low grade: 43 years • Median age with intermediate grade: 34 • Median age with high grade: 29 Angiosarcoma
Treatment: surgery with wide uninvolved margins • Prognosis: • Approximately 25% develop local recurrence • Approximately 60% develop distant metastasis • Most common sites of metastasis: lung, liver, skin and bone Angiosarcoma
45 year old female • Firm palpable mobile painless mass Case 5: Clinical history
Fibroepithelial lesion with cellular stroma • Intracanalicular pattern with “leaf-like” projection of cellular stroma • Easily identified mitotic figures Case 5: Histopathology
Case 5 Diagnosis:Phyllode Tumor Low grade malignant (Borderline)
Uncommon lesions: < 1% of breast tumors • Clinical presentation: • Reported in patients age range 10-86 years • Mean age: 45 years (aprox 20 years older than FA) • Firm, palpable mass; may have recent growth • Gross pathology • Firm bulging, gray-tan tissue, well circumscribed and non-encapsulated • Average size: 4-5 cm • Malignant PT may have foci of degeneration, encores or infarction Phyllodes Tumor (PT)
Grading: 3-tiered systems based on • Degree of cellularity • Stromal cell pleomorphism • Stromal mitotic count • Tumor border (circumscribed vs. invasive) • Stromal overgrowth • Presence of heterologous sarcomatous elements • Differential diagnosis: • Benign PT vs. fibroadenoma • Malignant PT vs. sarcoma and metaplastic tumors Phyllodes Tumor (PT)
Phyllodes Tumor (PT) WHO classification of tumors of the breast. 4th edition. 2012
Prognosis • Local recurrence occurs irrespective of grade and is most strongly associated with adequacy of surgical margins • Rate of metastasis: • Benign (never?) • Borderline ~ 4% • Malignant ~ 22% • Sarcomatous elements more likely to metastasize • Most common site of metastasis: lungs, pleura and bone Phyllodes Tumor (PT)
31 year old female • Family history of breast cancer in mother • Firm palpable painless breast mass Case 6: Clinical History
Pleomorphic tumor cells with syncytial growth pattern • High mitotic rate • Prominent lymphoplasmacytic response, particular at periphery • Pushing type border • Neutrophils (present within areas of tumor degeneration) Case 6: Histopathology
Defined by a constellation of histopathologic finding. Medullary carcinoma MUST have: • Lymphoplasmacytic reaction • Microscopic circumscription (smooth rounded pushing tumor border • Syncytial growth pattern • Poorly differentiated nuclear grade and high mitotic rate Medullary carcinoma MAY have: • Associated intraductal carcinoma • Metaplastic change (squamous) • Cystic degeneration or necrosis • Majority are triple negative for ER, PR and Her2 Medullary Carcinoma
Clinical presentation • Less than 5% of mammary carcinomas • Younger age: majority less than 50, mean = 45 years • Rare in males, rarely bilateral • Well circumscribed border by imaging • Gross presentation • Pale brown or tan bulging tumor • Circumscribed border with internal nodularity • May show cystic degeneration Medullary Carcinoma
Tumors with some but not all of the histologic features of medullary: • “Invasive ductal carcinoma with medullary features” • “Atypical medullary carcinoma” • Prognosis: Slightly better/ no better than invasive ductal carcinoma, NOS NOT medullary carcinoma
Prognosis • Favorable prognosis compared to other mammary carcinoma matched by stage Medullary Carcinoma Ridolfi, RL (10/1977). "Medullary carcinoma of the breast: a clinicopathologic study with 10 year follow-up". Cancer(0008-543X), 40(4), p.1365.
36-year-old female • Well-circumscribed right breast mass Case 7: Clinical history
Well circumscribed lesion • Lobular arrangement • Fibrous (pseudoangiomatous stromal hyperplasia) PASH-like stroma • Adipose tissue within the lesion Case 7: Histopathology
Differential diagnosis • Nodular PASH • Hamartoma • Fibroadenoma Case 7: differential diagnosis