Download
1 / 11
350 likes | 1.93k Views
Premalignant lesions of the cervix. Applied anatomy. Cervical intraepithelial neoplasia. It is a continuum from atypia to HSIL Confined to epithelium Thus non-invasive Thus a precursor of cervical cancer Pathologically described as CIN 1-3

E N D
Cervical intraepithelial neoplasia • It is a continuum from atypia to HSIL • Confined to epithelium • Thus non-invasive • Thus a precursor of cervical cancer • Pathologically described as CIN 1-3 • Of CIN1: most will regress. Of CIN 2: about a third will regress. Of CIN 3: ALL WILL PROGRESS TO CaCx
Epidemiology • Disease of sexually active women • Caused by high risk types of HPV namely 16, 18 and also 31,33,48, 52 and some other types • Epidemiological risk factors: early age of first coitus, multiple partners, smoking, immune suppression • Concerns: long term use of OC, multiple pregnancies, poor nutritional status
Prevalence • USA data: up to 80% of college graduates are HPV+ • By age 30: rate down to 30% HPV + • About 15% of women will have abnormal cytology • Every year in SA >20 new cases of CaCx per 100 000 women • As common as (or more common than) breast cancer
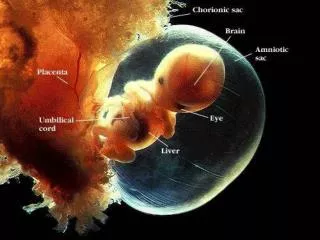
Pathogenesis • Pubertal developments: E leads to outgrowth of columnar epithelium: Exposed SCJ: leads to METAPLASIA • If HPV present: DYSPLASIA • Typically HPV -> atypia -> LSIL -> HSIL • Majority will regress but not all and not much from HSIL • Transmission time varies and can be years
Clinically • Mean age 30 (SA screening policy: will miss many; ? Role of HIV) • Mainly asymptomatic, may have PCB • Cx may appear normal or have a red lesion • COLPOSCOPY with acetic acid allows detection of abnormal area (acetowhite) -> biopsy (diagnosis made histologically)
Management of patient with abnormal smears • See flow diagram (is in GEP and textbook) • Preferred option is “one step” management where patients with abnormal smears are referred for colposcopy and also LLETZ at the same visit • This may be excessive for LSIL unless repeated or have follow-up problems
Treatment methods • Local destruction: cryotherapy, laser • Local excision: LLETZ, cone biopsy • Surgical options: hysterectomy (uncommonly) • LLETZ is current first choice management with >95% effectiveness and very few complications and side effects • Bi-to annual cytology for follow-up
Outcomes • If left untreated: • HPV, LSIL: most will regress • HSIL: all will probably develop CaCx over time • If HSIL is treated: <5% risk for recurrence (and then esp. when HIV+) • If treated and followed: <<1% risk for later CaCx
Counselling issues • Very hard to trace original source of HPV – not worth the trouble • Normal PAP smear result is good but follow-up screening should be performed • Male partner: most will have HPV but few will develop visible lesions (and then usually warts)