Download
1 / 159
1.63k likes | 2.02k Views
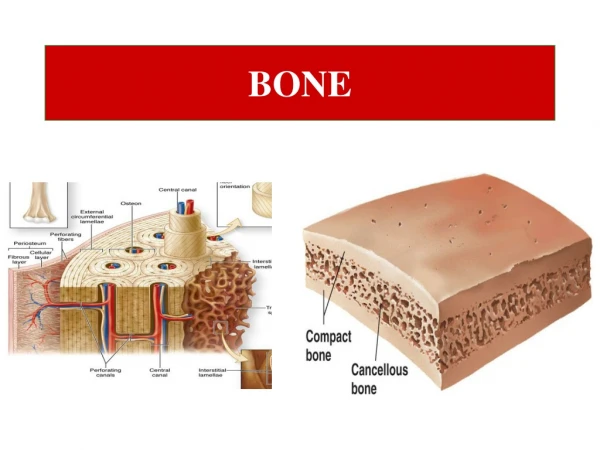
Bone . Bone . Organic matrix( 35%)- cells & proteinaceous osteoid Inorganic elements( 65%)-calcium hydroxyapatite , 99% of body’s ca- 85% of P- 65% of Na and Mg Remodeling: constant breakdown & renewal which the net effects may be bone maintenance, bone loss or bone deposition.

E N D
Bone Organic matrix( 35%)- cells & proteinaceousosteoid Inorganic elements( 65%)-calcium hydroxyapatite, 99% of body’s ca- 85% of P- 65% of Na and Mg Remodeling: constant breakdown & renewal which the net effects may be bone maintenance, bone loss or bone deposition
Bone diseases Congenital diseases Acquired diseases Fractures Osteonecrosis Osteomyelitis Tumors
Developmental anomalies localized problems in migration of mesenchymal cells & formation of condensations, dysostoses Isolated sporadic lesion or a component of a complex syndrome More common lesions Aplasia- congenital absence of a digit or rib Formation of extra bones- supernumerary digits or ribs Abnormal fusion of bones- premature closure of cranial sutures or congenital fusion of ribs
Mutations Interfere with bone or cartilage formation, growth, and/or maintenance of normal matrix components More diffuse defects Dysplasia osteodysplasia, chondrodysplasia
Other genetic metabolic disorders Not usually thought of as primary skeletal diseases, eg; mucopolysaccharidoses like Hurler syn
Osteogenesisimperfecta(brittle bone disease) A group of hereditary disorders caused by defective synthesis of type I collagen Gene mutations in coding sequences for α1 or α2 chains, quality or quantity( premature degradation, dominant negative mutation ) Most, AD Extraskeletal manifestations: skin, joints, eyes….
OI Too little bone, extreme skeletal fragility Four major subtypes, extremely broad range of clinical outcome Type I- normal lifespan, fractures during childhood, blue sclera, hearing loss, small misshapen teeth Type II-fatal
Achondroplasia Activating Point mutation in FGF receptor3 Activation of receptor Inhibits chondrocyte proliferation Impaired long bone growth
Achondroplasia AD Spontaneous mutation( many cases ) Affected individuals are typically heterozygotes Homozygotes die soon after birth because of abnormalities in chest development & respiratory failure
Clinical findings Most common form of dwarfism Affects all bones that form from a cartilaginous framework Most conspicuous changes: marked disporportionate shortening of proximal extremities, bowing of the legs, lordotic posture Cartilage growth plate: disorganized & hypoplastic
Osteopetrosis A group of rare genetic disorders characterized by reduced osteoclast-mediated bone resorption, defective bone remodeling Several variants, most common: 1- AD adult form with mild clinical manifestations 2- AR infantile with a severe/ lethal phenotype
Osteopetrosis Causing defects Those that disturb osteoclast function Those that interfere with osteoclast formation & differentiation
osteoclast dysfunction Bone resorption through osteocalsts: decalcification by proton pump and degrading enzymes also activation of mediators Nature of osteoclast dysfunction unknown in many cases Carbonic anhydrase II deficiency results in reduced bone demineralization( required for osteoclast H+ excretion) Proton pump deficiency Chloride channel defect
Clinical findings Fractures Cranial nerve problems Recurrent infections( diminished hematopoiesis ) Hepatosplenomegaly Bone marrow transplant
Acquired diseases of bone development Nutritional deficiencies( vit c, vit d) Primary & secondary hyperparathyroidism Osteoporesis Paget disease Rickets & osteomalacia
Osteoporosis Increased porosity of skeleton resulting from reduced bone mass, increase in bone fragility & fx Localized to a bone or region or generalized Most common forms: senile, postmenopausal Bone loss generally occurs in areas containing abundant cancelloues bone so more pronounced in spine & femoral neck
Paget disease Gain in bone mass but newly formed bone is disordered & lacks strength Repetitive episodes of regional osteoclastic activity & bone resorption- followed by exuberant bone formation- finally by exhaustion of cellular activity Osteolytic stage, mixed osteoclastic- osteoblastic stage, osteosclerotic stage Age: mid adulthood Marked variation in prevalence in different populations
Morphology Lytic phase- numerous & large osteoclasts Mixed phase- prominent osteoblasts, marrow replaced by loose connective tissue Mosaic pattern( pathogonomichistologic feature )
Pathogenesis Paramyxovirus infection IL-1 secretion from infected cells, M-CSF activate osteoclasts Other suggested mechanism: intrinsic hyperresponsiveness of osteoclasts to activating agents as, vitD & RANK ligand.
Clinical course Monostotic 15% ( tibia, ilium, femur, skull, vertebra, humerus ) Polyostotic ( pelvis, spine, skull ) axial skeleton or proximal femur , 80% of cases Ribs, fibula & small bones of hands & feet : unusual Most cases are mild & discovered incidentally Elevation in serum ALKP & increased urinary excretion of hydroxyproline
Manifestations Warmth of overlying skin & subcutis In extensive polyostotic disease high output congestive heart failure In proliferative phase of skull disease, nerve impigment headache & visual and auditory disturbances Back pain with vertebral lesions, fx & nerve root compression Deformity of long bones of leg Sarcoma in 1% of patients parallel to lesions except vertebra
Rickets & Osteomalacia Defective bone mineralization
PTH Osteoclast activation( increased RANKL production by osteoblasts ) Increased resorption of ca by renal tubules Increased urinary excretion of phosphate Increased synthesis of 1,25(OH)2 vitD by kidneys Net result: elevation in serum ca, inhibiting PTH
Hyperparathyroidism Significant skeletal changes related to unabated osteoclast activity Entire skeleton is affected, some sites may be more severely affected PTH is directly responsible for bone changes in primary but additional influences contribute in secondary Inadequate 1,25(OH)2 vitD synthesis in chronic renal failure
Brown tumor Osteitisfibrosacystica
Healing Blood coagulum recruit inflammatory cells, fibroblast & endothelium Release of cytokines from plts & inflammatory cells Activate bone progenitor cells Soft tissue callus, within a week Deposition of woven bone Chondroblasts Early repair process peak within 2-3 wks Bony callus Weight bearing leads to resorption of callus from nonstressed sites
Disrupting factors Displaced & comminuted fractures Inadequate immobilization nlconstiuents do not form Too much motion along fx gap Infection Inadequate levels of ca or p, vit deficiencies, systemic infection, diabetes, vascular insufficiency
Mechanisms Vascular compression or disruption Steroid administration Thromboembolic disease Primary vessel disease (eg; vasculitis )
Osteonecrosis Cortex, usually not affected Subchondral infarcts Medullary infarcts
Osteomyelitis Pyogenic tuberculous
Pyogenicosteomyelitis Routes Organisms: staph aureus, E-coli and strep group B, salmonella, mixed bacterial infections No organism isolated, 50% of cases Associated suppurative arthritis in infants Sequestrum Involucrum Subperiosteal abscess and draining sinus After the 1st week of infection chronic inflammatory cell become numerous ¼ of cases do not resolve and persist as chronic infection
Complications of chronic OM Acute flare ups Pathologic fx Secondary amyloidosis Endocarditis Sepsis SCC Osteosarcoma, rarely