Download
1 / 31
450 likes | 1.51k Views
Viral Meningitis Dr Fiona McGill Dr Fiona McGill is a specialist registrar in infectious diseases and medical microbiology in the Yorkshire and Humber Deanery and a clinical research fellow with the Liverpool Brain Infections Group at the University of Liverpool.

E N D
Viral Meningitis Dr Fiona McGill Dr Fiona McGill is a specialist registrar in infectious diseases and medical microbiology in the Yorkshire and Humber Deanery and a clinical research fellow with the Liverpool Brain Infections Group at the University of Liverpool. Edited by Prof Tom Solomon and Dr Agam Jung • Viral Meningitis • Learning Objectives • Overview • Causes of aseptic meningitis • Epidemiology • Clinical Features • Investigations • Lumbar puncture • Blood tests • Viral meningitis vs encephalitis • Treatment • Enteroviral meningitis • Herpes meningitis • VSV meningitis • HIV infection • Complications • Key points • Summary • Clinical scenarios • Self assessment Viral meningitis is a common illness in the UK and abroad. It is often quoted as being a benign, self-limiting illness. Although the disease is rarely fatal in adults, there is mounting evidence that it can cause important complications in certain patients. This session will present the current evidence and clinical guidelines to guide the management of patients with viral meningitis. Adapted with kind permission from: McGill F, Michael B, Solomon T. Viral meningitis in adults – a practical approach. BMJ Learning 2012
Learning Objectives • After completing this module, you should know: • That viral meningitis is a common problem in the UK • The important causes of aseptic meningitis • How to manage a patient with meningism and a raised lymphocyte count in their cerebrospinal fluid • How to differentiate between viral and bacterial causes of meningitis • The difference between viral meningitis and viral encephalitis • The possible outcomes for patients with viral meningitis. • Viral Meningitis • Learning Objectives • Overview • Causes of aseptic meningitis • Epidemiology • Clinical Features • Investigations • Lumbar puncture • Blood tests • Viral meningitis vs encephalitis • Treatment • Enteroviral meningitis • Herpes meningitis • VSV meningitis • HIV infection • Complications • Key points • Summary • Clinical scenarios • Self assessment
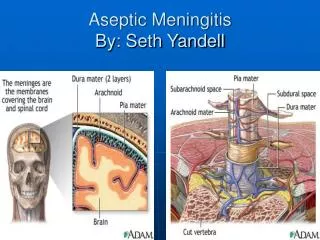
Overview • Meningitis is inflammation of the meninges which surround the brain and spinal cord. It is normally due to an infection and can be caused by viruses, bacteria or fungi. This module focuses on viral meningitis. • Viral meningitis is an important cause of morbidity. You must be able to differentiate viral meningitis from both bacterial meningitis and viral encephalitis. This is because bacterial meningitis and viral encephalitis are associated with a higher mortality and morbidity rate than viral meningitis. • You should not use the terms viral meningitis and aseptic meningitis interchangeably. In a patient with symptoms of meningism, aseptic meningitis is defined as: • a cerebrospinal fluid (CSF) with a white cell count of over 5 x 106/L (>5 cells/mm3) with a negative bacterial culture of the CSF • Viral Meningitis • Learning Objectives • Overview • Causes of aseptic meningitis • Epidemiology • Clinical Features • Investigations • Lumbar puncture • Blood tests • Viral meningitis vs encephalitis • Treatment • Enteroviral meningitis • Herpes meningitis • VSV meningitis • HIV infection • Complications • Key points • Summary • Clinical scenarios • Self assessment RIGHT: The meninges of the central nervous system consist of the dura mater, arachnoid and pia mater
Causes of Aseptic Meningitis Viral meningitis is a type of aseptic meningitis. Aseptic meningitis has many other causes in addition to viruses. Some common and less common causes of aseptic meningitis are shown in the below table. • Viral Meningitis • Learning Objectives • Overview • Causes of aseptic meningitis • Epidemiology • Clinical Features • Investigations • Lumbar puncture • Blood tests • Viral meningitis vs encephalitis • Treatment • Enteroviral meningitis • Herpes meningitis • VSV meningitis • HIV infection • Complications • Key points • Summary • Clinical scenarios • Self assessment Causes of aseptic meningitis (adapted from Meningitis, Chapter 41, Brain’s Diseases of the Nervous System by T. Solomon).
Epidemiology Although viral meningitis is a notifiable disease, the exact incidence is unknown as it is probably under-diagnosed and under-reported. In England and Wales in 2009, 260 episodes of viral meningitis were notified to the Health Protection Agency (HPA). More detailed epidemiological studies have estimated that the true rate of disease may be about 10 to 14 times this number. So the number of notified episodes is likely to be a gross underestimate. In the UK, the most common viruses that cause viral meningitis are the enteroviruses and the herpes viruses. Other viruses, such as enterovirus serotype 71, may be the cause in people who are on holiday or resident in other countries. Some other tropical viruses can cause an aseptic meningitis, but more frequently cause encephalitis than meningitis. These include dengue, Japanese encephalitis, and West Nile virus. These are beyond the scope of this module. • Viral Meningitis • Learning Objectives • Overview • Causes of aseptic meningitis • Epidemiology • Clinical Features • Investigations • Lumbar puncture • Blood tests • Viral meningitis vs encephalitis • Treatment • Enteroviral meningitis • Herpes meningitis • VSV meningitis • HIV infection • Complications • Key points • Summary • Clinical scenarios • Self assessment
Clinical Features • Patients with viral meningitis present with signs of meningeal irritation, termed ‘meningism’, and fever. Meningism refers to neck stiffness, headache and photophobia. Fever is often the most common presenting feature and neck stiffness the least common,but viral meningitis can and does occur in the absence of fever. Other non-specific symptoms are often also present, including diarrhoea and vomiting, muscle pain, and sore throat. • There is usually no reduced conscious level in patients with viral meningitis. An alteration in conscious level suggests an alternative diagnosis, for example: • Bacterial meningitis • Encephalitis (inflammation of the brain substance) • Encephalopathy due to infection outside the central nervous system, which is termed ‘septic encephalopathy’. • Sometimes a patient does not present clearly with either meningitis or encephalitis and this is termed meningoencephalitis, implying involvement of the brain substance as well as the meninges. • Viral Meningitis • Learning Objectives • Overview • Causes of aseptic meningitis • Epidemiology • Clinical Features • Investigations • Lumbar puncture • Blood tests • Viral meningitis vs encephalitis • Treatment • Enteroviral meningitis • Herpes meningitis • VSV meningitis • HIV infection • Complications • Key points • Summary • Clinical scenarios • Self assessment
Approach to Investigation • There are several British and international guidelines on meningitis and encephalitis in adults from: • The British Infection Association (BIA) • The BIA and Association of British Neurologists (the National Encephalitis Guideline). • Infectious Diseases Society of America • This section outlines the best approach to investigations, as recommended by these guidelines. • Viral Meningitis • Learning Objectives • Overview • Causes of aseptic meningitis • Epidemiology • Clinical Features • Investigations • Lumbar puncture • Blood tests • Viral meningitis vs encephalitis • Treatment • Enteroviral meningitis • Herpes meningitis • VSV meningitis • HIV infection • Complications • Key points • Summary • Clinical scenarios • Self assessment
Lumbar Puncture I • It is difficult to differentiate viral meningitis from bacterial meningitis on clinical grounds alone, as patients can present with meningism and fever in both diseases. Therefore a lumbar puncture is necessary to confirm the diagnosis of meningitis and look for a causative agent. • Unless there are specific clinical contraindications to lumbar puncture, a CT brain is NOT necessary before proceeding to lumbar puncture. • You should send CSF to the laboratory and request the following tests on it: • Microscopy and culture (2 bottles) – this will also give the white and red cell counts with a white cell differential • Protein • Glucose (you must also perform a simultaneous blood glucose) • You should send a further sample of CSF to the laboratory for storage. If an increase in lymphocytes (lymphocytosis) is identified, you should then send this CSF for PCR (polymerase chain reaction). This will look for causative viruses. Depending on the results from the CSF, further tests may be necessary. • Viral Meningitis • Learning Objectives • Overview • Causes of aseptic meningitis • Epidemiology • Clinical Features • Investigations • Lumbar puncture • Blood tests • Viral meningitis vs encephalitis • Treatment • Enteroviral meningitis • Herpes meningitis • VSV meningitis • HIV infection • Complications • Key points • Summary • Clinical scenarios • Self assessment
Lumbar Puncture II • Features that suggest viral meningitis include: • A raised white cell count in the CSF (>5 cells/mm3 in adults) with a predominance of lymphocytes (although neutrophils may predominate if the lumbar puncture is done early in the disease) • Mildly raised protein (0.5 to 1 g/L) • Normal ratio of glucose in CSF:blood (>66%) (Most textbooks quote 66% as the normal ratio, but only values of <50% are likely to be clinically important, e.g. bacterial meningitis.) • PCR is now the gold standard for diagnosing the causative agent in viral meningitis. Most laboratories in the UK will test for enteroviruses, herpes simplex viruses (HSV) types 1 and 2, and varicella zoster virus (VZV). Some laboratories also test for parechoviruses and other less common viruses. • No cause is found in around 35% of patients with lymphocytic meningitis • Viral Meningitis • Learning Objectives • Overview • Causes of aseptic meningitis • Epidemiology • Clinical Features • Investigations • Lumbar puncture • Blood tests • Viral meningitis vs encephalitis • Treatment • Enteroviral meningitis • Herpes meningitis • VSV meningitis • HIV infection • Complications • Key points • Summary • Clinical scenarios • Self assessment
Lumbar Puncture III Normal white cell count in the CSF It is sometimes possible to detect virus in the CSF even if there is no elevation in white cells. This does not always mean that the patient has meningitis. You need to look at the patient’s clinical features to see if it is possible that there could be neurological infection without a rise in white cells in the CSF. For example, a patient with shingles but no signs of meningism may have detectable levels of VZV in their CSF despite the white cell count in their CSF being normal. This patient may not necessarily have meningitis. An immunocompromised patient with neck stiffness and photophobia may have the same CSF findings as the patient with shingles, but is more likely to have meningitis. • Viral Meningitis • Learning Objectives • Overview • Causes of aseptic meningitis • Epidemiology • Clinical Features • Investigations • Lumbar puncture • Blood tests • Viral meningitis vs encephalitis • Treatment • Enteroviral meningitis • Herpes meningitis • VSV meningitis • HIV infection • Complications • Key points • Summary • Clinical scenarios • Self assessment
Other Investigations Blood tests The white cell count and C-reactive protein (CRP) may be normal or mildly raised in patients with viral meningitis. HIV test Aseptic meningitis can be a presenting feature of HIV seroconversion. So you should offer an HIV test to all patients with aseptic meningitis. • Viral Meningitis • Learning Objectives • Overview • Causes of aseptic meningitis • Epidemiology • Clinical Features • Investigations • Lumbar puncture • Blood tests • Viral meningitis vs encephalitis • Treatment • Enteroviral meningitis • Herpes meningitis • VSV meningitis • HIV infection • Complications • Key points • Summary • Clinical scenarios • Self assessment
Differentiating encephalitis and meningitis I • There can be confusion between encephalitis and meningitis when a patient has a lymphocytic CSF. The clinical picture will help you to differentiate between the two. Features that suggest involvement of the brain substance (parenchyma) and therefore encephalitis are: • Focal neurological weakness • Seizures or movement disorder • Change in personality, behaviour, cognition or consciousness • In a patient with a lymphocytic CSF and an impaired conscious level, you should start treatment for presumed herpes simplex encephalitis. Herpes simplex encephalitis is a medical emergency and prompt treatment with aciclovir has been shown to reduce mortality and morbidity. You may wish to consider antibiotics as well until the definitive diagnosis is made. • Other causes of a lymphocytic CSF include tuberculosis, listeriosis, partially treated bacterial meningitis and all the causes of aseptic meningitis. • Viral Meningitis • Learning Objectives • Overview • Causes of aseptic meningitis • Epidemiology • Clinical Features • Investigations • Lumbar puncture • Blood tests • Viral meningitis vs encephalitis • Treatment • Enteroviral meningitis • Herpes meningitis • VSV meningitis • HIV infection • Complications • Key points • Summary • Clinical scenarios • Self assessment
Differentiating encephalitis and meningitis II • Viral Meningitis • Learning Objectives • Overview • Causes of aseptic meningitis • Epidemiology • Clinical Features • Investigations • Lumbar puncture • Blood tests • Viral meningitis vs encephalitis • Treatment • Enteroviral meningitis • Herpes meningitis • VSV meningitis • HIV infection • Complications • Key points • Summary • Clinical scenarios • Self assessment
Treatment There are currently no treatments of proven benefit for the common causes of viral meningitis. Some clinicians treat patients who have herpes meningitis with aciclovir or valaciclovir, but to date, there have been no trials to support or refute this practice. Treatment should be supportive and reassuring. As viral meningitis is often difficult to differentiate from bacterial meningitis based on clinical features alone, it is possible that the patient will be on antibiotics before the viral aetiology is determined. Once the diagnosis has been established as viral meningitis, you should stop antibiotics, if they have been prescribed, and prioritise discharge from hospital. If HSV-2 is diagnosed, you should consider referring the patient to a sexual health clinic. The most common specific causes of viral meningitis are considered on the following slides. • Viral Meningitis • Learning Objectives • Overview • Causes of aseptic meningitis • Epidemiology • Clinical Features • Investigations • Lumbar puncture • Blood tests • Viral meningitis vs encephalitis • Treatment • Enteroviral meningitis • Herpes meningitis • VSV meningitis • HIV infection • Complications • Key points • Summary • Clinical scenarios • Self assessment
Enteroviral Meningitis I In most studies, enteroviruses are the most common cause of viral meningitis. Diagnosis has improved greatly since the widespread use of PCR. By using molecular techniques to obtain a definitive diagnosis, the length of hospital stay and duration of antibiotics can both be reduced. Enteroviruses are a group of viruses that include polioviruses, echoviruses, coxsackie viruses and the numbered enteroviruses. Viral meningitis is caused mainly by the coxsackie viruses and echoviruses. As the name suggests, enteroviruses are carried in the gastrointestinal tract and can be found on PCR of stool samples and throat swabs. The viruses tend to be carried in the throat during the acute episode. So if a patient with symptoms of meningism and raised white cells in their CSF has a positive throat swab for enterovirus, this is strongly suggestive as the cause of their meningitis. However, the same is not true of stool samples, as the virus can be excreted in the stool in well individuals as well as those with meningitis. These tests do not confirm the cause of meningitis, so you must perform a lumbar puncture for PCR analysis of the CSF. • Viral Meningitis • Learning Objectives • Overview • Causes of aseptic meningitis • Epidemiology • Clinical Features • Investigations • Lumbar puncture • Blood tests • Viral meningitis vs encephalitis • Treatment • Enteroviral meningitis • Herpes meningitis • VSV meningitis • HIV infection • Complications • Key points • Summary • Clinical scenarios • Self assessment
Enteroviral Meningitis II There is a seasonal variation in enteroviral meningitis, with most cases occurring in the summer/autumn in the Northern Hemisphere. Most immunocompetent adults recover from enteroviral meningitis without complication. But there is some evidence that patients may be left with neuropsychological dysfunction, for example, problems with attention or cognition. There is also evidence that enteroviral meningitis can leave people with fatigue and sleep problems. Enteroviralmeningoencephalitis in neonates can be fatal. There is no current, licensed treatment for enteroviral meningitis. • Viral Meningitis • Learning Objectives • Overview • Causes of aseptic meningitis • Epidemiology • Clinical Features • Investigations • Lumbar puncture • Blood tests • Viral meningitis vs encephalitis • Treatment • Enteroviral meningitis • Herpes meningitis • VSV meningitis • HIV infection • Complications • Key points • Summary • Clinical scenarios • Self assessment
Herpes Virus Meningitis Several herpes viruses can cause meningitis. HSV-2 is normally the most common (one study found VZV to be the most common). Although a common casue of encephalitis, HSV-1 is an uncommon cause of aseptic meningitis. Outside the perinatal period, HSV-2 is normally acquired sexually. Most people with HSV-2 meningitis do not have concurrent genital herpes and usually have no history of such either. Recurrent lymphocytic meningitis, also known as Mollaret’s meningitis, is a rare disease that is estimated to have a prevalence of 2.7 per 100,000 population. HSV-2 is the most common cause of recurrent lymphocytic meningitis, being responsible for 84% of recurrent meningitis in one study. However, most patients who have one episode of HSV-2 meningitis do not go on to have a recurrence. Although aciclovir is used for other illnesses caused by herpes viruses, there is currently no strong evidence for or against its use in herpes meningitis. Treatment of herpes meningitis, including the use of aciclovir, varies greatly within the UK and the US, and there is a need for well conducted clinical trials. A recent trial looked at the role of valaciclovir in the prevention of recurrent episodes of HSV-2 meningitis, but no benefit was shown. • Viral Meningitis • Learning Objectives • Overview • Causes of aseptic meningitis • Epidemiology • Clinical Features • Investigations • Lumbar puncture • Blood tests • Viral meningitis vs encephalitis • Treatment • Enteroviral meningitis • Herpes meningitis • VSV meningitis • HIV infection • Complications • Key points • Summary • Clinical scenarios • Self assessment
Varicella Zoster Virus Meningitis Meningitis caused by varicella zoster virus (VZV) can occur during either primary infection with the virus (chickenpox) or reactivation (shingles), or after the live vaccine. Aseptic meningitis has been shown to be the most common neurological manifestation of VZV infection. VZV meningitis presents with the classic symptoms of meningism, although less frequently than in other forms of viral meningitis according to one study. Rash is also more common with VZV than with herpes or enteroviruses. But VZV meningitis can occur in the absence of skin lesions. Aciclovir has activity against VZV, but there are no trials to support its use in the setting of meningitis. But if there is clinical or radiographic evidence of meningoencephalitis in the patient, experts recommend the use of aciclovir. • Viral Meningitis • Learning Objectives • Overview • Causes of aseptic meningitis • Epidemiology • Clinical Features • Investigations • Lumbar puncture • Blood tests • Viral meningitis vs encephalitis • Treatment • Enteroviral meningitis • Herpes meningitis • VSV meningitis • HIV infection • Complications • Key points • Summary • Clinical scenarios • Self assessment Right: The rash of Herpes Zoster infection
HIV and neurological illness HIV is an important cause of neurological illness, both due to direct involvement, as in HIV seroconversion, and secondary to opportunistic infections, such as VZV and cryptococcus. Aseptic meningitis can be caused by HIV, especially at the time of seroconversion. In one study, symptoms of meningitis occurred in 24% of patients presenting with primary HIV infection. This study also showed that most of these patients presenting with typical symptoms of primary HIV infection were not diagnosed at the initial medical encounter. Therefore, you should offer an HIV test to all patients with aseptic meningitis. Other studies have also shown that aseptic meningitis or encephalitis can present in established HIV infection as well as primary disease. • Viral Meningitis • Learning Objectives • Overview • Causes of aseptic meningitis • Epidemiology • Clinical Features • Investigations • Lumbar puncture • Blood tests • Viral meningitis vs encephalitis • Treatment • Enteroviral meningitis • Herpes meningitis • VSV meningitis • HIV infection • Complications • Key points • Summary • Clinical scenarios • Self assessment
HIV and neurological illness In the UK, about one third of people who have HIV are currently undiagnosed and unaware of their infection. In addition, HIV is still often diagnosed late. In a recent British HIV Association (BHIVA) audit, over half of patients had a CD4 count of less than 350 cells/mm3 when diagnosed. A CD4 count of 350 cells/mm3 is the threshold below which treatment for HIV should be started. Many patients who were diagnosed late had had a previous, missed opportunity for HIV testing. In a previous audit of mortality in patients with HIV, a quarter of deaths were reported as being due to the diagnosis of HIV being made too late for effective treatment. It is for these reasons that national guidelines on HIV testing have been produced which indicate when to offer an HIV test. These can be found by following the below link. • Viral Meningitis • Learning Objectives • Overview • Causes of aseptic meningitis • Epidemiology • Clinical Features • Investigations • Lumbar puncture • Blood tests • Viral meningitis vs encephalitis • Treatment • Enteroviral meningitis • Herpes meningitis • VSV meningitis • HIV infection • Complications • Key points • Summary • Clinical scenarios • Self assessment
Complications Viral meningitis is often reported as a benign, self-limiting illness. But there is mounting evidence that the disease may have longer term effects, such as cognitive dysfunction, sleep disturbances and persistence of headaches. One study showed that patients who had viral meningitis have significantly lower global cognitive scores than control patients. Another study showed that headache occurs in up to 34% of patients. Memory, attention and speed of cognitive and psychomotor performance are the domains most affected. No studies have been conducted into whether these complications reduce over time. HSV-2 and other viruses can cause recurrent episodes of meningitis (Mollaret’s meningitis). • Viral Meningitis • Learning Objectives • Overview • Causes of aseptic meningitis • Epidemiology • Clinical Features • Investigations • Lumbar puncture • Blood tests • Viral meningitis vs encephalitis • Treatment • Enteroviral meningitis • Herpes meningitis • VSV meningitis • HIV infection • Complications • Key points • Summary • Clinical scenarios • Self assessment
Key Points I • Viral meningitis is a common problem in the UK and can have important complications • Herpes viruses (including HSV-2) and the enteroviruses are the most common causes of viral meningitis in the UK • Viral meningitis and viral encephalitis are usually separate entities and the diagnostic approaches and management are different • You should offer an HIV test to all adult patients with aseptic meningitis • By diagnosing the specific (viral) pathogen causing the symptoms, you can reduce the length of hospital stay and amount of inappropriate antibiotics given • Viral Meningitis • Learning Objectives • Overview • Causes of aseptic meningitis • Epidemiology • Clinical Features • Investigations • Lumbar puncture • Blood tests • Viral meningitis vs encephalitis • Treatment • Enteroviral meningitis • Herpes meningitis • VSV meningitis • HIV infection • Complications • Key points • Summary • Clinical scenarios • Self assessment
Key Points II • Below are some key clinical tips to bear in mind in the approach to viral meningitis: • You should arrange a lumbar puncture for all patients with suspected meningitis, unless there are clinical contraindications, in order to differentiate bacterial from viral causes • A CT head before a lumbar puncture is normally unnecessary and unhelpful • You should refer patients with HSV-2 meningitis to a centre for sexual health • You should notify all episodes of viral meningitis to your local Health Protection Unit • Viral Meningitis • Learning Objectives • Overview • Causes of aseptic meningitis • Epidemiology • Clinical Features • Investigations • Lumbar puncture • Blood tests • Viral meningitis vs encephalitis • Treatment • Enteroviral meningitis • Herpes meningitis • VSV meningitis • HIV infection • Complications • Key points • Summary • Clinical scenarios • Self assessment
Summary • You should now know: • That viral meningitis is a common problem in the UK • The important causes of aseptic meningitis • How to manage a patient with meningism and a raised lymphocyte count in their cerebrospinal fluid • How to differentiate between viral and bacterial causes of meningitis • The difference between viral meningitis and viral encephalitis • The possible outcomes for patients with viral meningitis. • Further resources • http://www.britishinfection.org/drupal/sites/default/files/MeningitisAlgorithm03.pdf • http://www.bhiva.org/documents/Guidelines/Testing/GlinesHIVTest08.pdf • http://www.meningitis.org/ • http://guidance.nice.org.uk/CG102/NICEGuidance/pdf/English • http://www.idsociety.org/IDSA/Site_Map/Guidelines/Patient_Care/IDSA_Practice_Guidelines/Infections_by_Organ_System/Central_Nervous_System_(CNS)/Bacterial_Meningitis.aspx • Viral Meningitis • Learning Objectives • Overview • Causes of aseptic meningitis • Epidemiology • Clinical Features • Investigations • Lumbar puncture • Blood tests • Viral meningitis vs encephalitis • Treatment • Enteroviral meningitis • Herpes meningitis • VSV meningitis • HIV infection • Complications • Key points • Summary • Clinical scenarios • Self assessment
Summary II • References • 1. Schmidt H, Cohrs S, Heinemann T, Goerdt C, Djukic M, Heimann B, et al. Sleep disorders are long-term sequelae of both bacterial and viral meningitis. Journal of Neurology, Neurosurgery and Psychiatry. 2006;77:554-8. • 2. Schmidt H, Heimann B, Djukic M, Mazurek C, Fels C, Wallesch CW, et al. Neuropsychological sequelae of bacterial and viral meningitis. Brain. 2006;129:333-45. • 3. Sittinger H, Muller M, Schweizer I, Merkelback S. Mild cognitive impairment after viral meningitis in adults. Journal of Neurology. 2002;249:554-60. • 4. Khetsuriani N, Quiroz ES, Holman R, Anderson LJ. Viral Meningitis-Associated Hospitalisations in the United States, 1988-1999. Neuroepidemiology. 2003;22:345-52. • 5. Landry ML, Greenwold J, Vikram HR. Herpes Simplex type-2 Meningitis: Presentation and Lack of Standardized Therapy. The American Journal of Medicine. 2009;122:688-91. • 6. Michael B, Sidhu M, Stoeter D, Roberts M, Beeching N, Bonington A, et al. Acute central nervous system infections in adults—a retrospective cohort study in the NHS North West region. QJM. [Original Paper]. 2010 24/07/2010;103:10. • 7. Rantakallio P, Leskinen M, Von Wendt L. Incidence and Prognosis of Central Nervous System Infections in a Birth Cohort of 12000 Children. Scand Journal of Infectious Diseases. 1986;18:287-94. • 8. Kupila L, Vuorinen T, Vainionpaa R, Hukkanen V, Marttila RJ, Kotilainen P. Etiology or aseptic meningitis and encephalitis in an adult population. Neurology. 2006;66:6. • 9. Solomon T. Meningitis. In: Donaghy M, editor. Brain's Diseases of the Nervous System. 12th ed: Oxford University Press; 2009. p. 1327-54. • 10. Chadwick D. Viral meningitis. Br Med Bull. 2005;75-76:1-14. • 11. Logan S, MacMahon E. Viral meningitis. BMJ. 2008;336:36-40. • 12. Brabazon ED, O'Farrell A, Murray CA, Finnegan P. Trends in viral meningitis hospitalisations and notifications in the North Eastern Health Board (1997 - 2001): a cause for concern? Irish Medical Journal. 2004;97(10):306-8. • 13. Rotbart HA. Enteroviral Infections of the Central Nervous System. Clinical Infectious Diseases. 1995;20:971-81. • Viral Meningitis • Learning Objectives • Overview • Causes of aseptic meningitis • Epidemiology • Clinical Features • Investigations • Lumbar puncture • Blood tests • Viral meningitis vs encephalitis • Treatment • Enteroviral meningitis • Herpes meningitis • VSV meningitis • HIV infection • Complications • Key points • Summary • Clinical scenarios • Self assessment
Summary III • References • 14. Ihekwaba UK, Kudesia G, McKendrick M. Clinical Features of Viral Meningitis in Adults: Significant Differences in Cerebrospinal Fluid Findings among Herpes Simplex Virus, Varicella Zoster Virus and Enterovirus Infections. Clinical Infectious Diseases. 2008;47:783-9. • 15. Desmond RA, Accortt NA, Talley L, Villano SA, Soong SJ, Whitley RJ. EnteroviralMeningitis:Natural history and Outcome of Pleconaril Therapy. Antimicrobial Agents and Chemotherapy. 2006;50(7):2409-14. • 16. Brivet FG, Ducuing S, Jacobs F, Chary I, Pompier R, Prat D, et al. Accuracy of Clinical Presentation for differentiating bacterial from viral meningitis in adults: a multivariate approach. Intensive Care Medicine. 2005;31:1654-60. • 17. Heyderman RS, Lambert HP, O'Sullivan I, Stuart JM, Taylor BL, Wall RA, et al. Early Management of Suspected Bacterial Meningitis and Meningococcal Septicaemia in Adults. Journal of Infection. 2003;46:75-7. • 18. Hasbun R, Abrahams J, Jekel J, Quagliarello VJ. Computed tomography of the Head before Lumbar Puncture in Adults with Suspected Meningitis. New England Journal of Medicine. 2001;345:1727-33. • 19. Solomon T, Hart I, Beeching N. Viral Encephalitis: A Clinician's guide. Practical Neurology. 2007;7:288-305. • 20. Jeffrey KJ, Bangham CRM. Recent Advances in the laboratory diagnosis of central nervous system infections. Current Opinion in Infectious Diseases. 1996;9:132-7. • 21. Jeffrey KJ, Read SJ. Diagnosis of viral infections of the Central nervous system: Clinical interpretation of PCR results. Lancet. 1997;349(9048):313-7. • 22. Nowak DA, Boehmer R, Fuchs HH. A retrospective clinical, laboratory and outcome analysis in 43 cases of acute aseptic meningitis. European Journal of Neurology. 2003;10:271-80. • 23. British HIV Association, British Association of Sexual Health and HIV, British Infection Society. UK National HIV Testing Guidelines for HIV testing 2008. 2008. • 24. Solomon T, MIchael BD, Smith PE, Sanderson F, Davies NWS, Hart I, et al. National ABN/BIA guideline for the management of encephalitis for adults. Journal of Infection. 2012;In press. • Viral Meningitis • Learning Objectives • Overview • Causes of aseptic meningitis • Epidemiology • Clinical Features • Investigations • Lumbar puncture • Blood tests • Viral meningitis vs encephalitis • Treatment • Enteroviral meningitis • Herpes meningitis • VSV meningitis • HIV infection • Complications • Key points • Summary • Clinical scenarios • Self assessment
Summary IV • References • 25. Tunkel AR, Hartman BJ, Kaplan SL, Kaufman BA, Roos KL, Scheld M, et al. Practice Guidelines for the management of Bacterial Meningitis. Clinical Infectious Diseases. 2004;39:1267-84. • 26. Smith J, Robinson J. Age-Specific Prevalence of Infection with herpes Simplex Types 2 and 1: A Global Review. Journal of Infectious Diseases. 2002;186 (Suppl1):S3-S28. • 27. Kallio-Laine K, Seppanen M, Kautiainen H, Lokki ML, Lappalainen M, Valtonen V, et al. Recurrent Lymphocytic Meningitis Positive for Herpes Simplex Virus Type 2. Emerging Infectious Diseases. 2009;15:1119-22. • 28. Chadwick D, Lever A. The impact of new diagnostic methodologies in the management of meningitis in adultsat a teaching hospital. QJM. 2002;95:663-70. • 29. Schuffenecker I, Mirand A, Antona D, Henquell C, Chomel JJ, Archimbaud C, et al. Epidemiology of human enterovirus 71 infections in France, 2000-2009. Journal of Clinical Virology. 2011;50:50-6. • 30. Skoldenberg B, Alestig K, Burman L, Forkman A, Lovgren K, Norrby R, et al. Acyclovir versus vidaribine in Herpes Simplex Encephalitis. The Lancet. 1984;324(8405):707-11. • 31. Kupila L, Vainionpaa R, Vuorinen T, Marttila RJ, Kotilainen P. Recurrent Lymphocytic Meningitis. Arch Neurol. 2004;61:1553-7. • 32. Koskiniemi M, Rantalaiho T, Piiparinen H, Bonsdorff CH von, Farkkila M, Jarvinen A, et al. Infections of the central nervous system of suspected viral origin: A colloaborative study from Finland. Journal of Neurovirology. 2001;7:400-8. • 33. Aurelius E, Franzen-Rohl E, Glimaker M, Akre O, Grillner L, Jorup-Ronstrom C, et al. Long term valacyclovir suppressive treatment after herpes simplex virus type-2 meningitis:a double blind, randomized controlled trial. Clinical Infectious Diseases. 2012;54:1304-13. • 34. Whitley RJ, Alford CA, HIrsch MS, Schooley RT, Luby JP, Aoki FY, et al. Vidarabine versus Acyuclovir Therapy in Herpes Simples Encephalitis. New England Journal of Medicine. 1986;314:144-9. • 35. McGrath N, Anderson NE, Croxson MC, Powell KF. Herpes Simplex encephalitis treated with acyclovir: diagnosis and long term outcome. Journal of Neurology, Neurosurgery and Psychiatry 1997;63:321-6. • Viral Meningitis • Learning Objectives • Overview • Causes of aseptic meningitis • Epidemiology • Clinical Features • Investigations • Lumbar puncture • Blood tests • Viral meningitis vs encephalitis • Treatment • Enteroviral meningitis • Herpes meningitis • VSV meningitis • HIV infection • Complications • Key points • Summary • Clinical scenarios • Self assessment
Summary V • 36. Fujimoto H, Asaoka K, Imaizumi T, Ayabe M, Shoji H, Kaji M. Epstein-Barr Virus Infections of the Central Nervous System. Internal Medicine. 2003;42(1):33-40. • 37. KOskiniemi M, Piiparinen H, Rantalaiho T, Eranko P, Farkkila M, Raiha K, et al. Acute Central Nervous System complications in varicella zoster virus infections. Journal of Clinical Virology. 2002;25:293-301. • 38. Pahud BA, Glaser CA, Dekker CL, Arvin AM, Schmid DS. Varicella Zoster Disease of the Central Nervous System: Epidemiological, Clinical and Laboratory Features 10 Years after the Introduction of the Varicella Vaccine. Journal of Infectious Diseases. 2011;203:316-23. • 39. Persson A, Bergstrom T, Lindh M, Namvar L, Studahl M. Varicella-zoster virus CNS disease - viral load, clinical manifestations and sequels. Journal of Clinical Virology. 2009;46:249-53. • 40. Schaker T, Collier AC, Hughes J, Shea T, Corey L. Clinical and Epidemiological Features of Primary HIV Infection. Annals of Internal Medicine. 1996;125(4):257-64. • 41. Villar del Saz S, Sued O, Falco V, Aguero F, Crespo M, Pumarola T, et al. Acute meningoencephalitis due to human inmmunodeficiency virus type 1 infection in 13 patients: clinical description and follow-up. Journal of neurovirology. 2008;14:474-9. • 42. Health Protection Agency, Infections. Cf. Testing times. HIV and other sexually transmitted infections in the United Kingdom:2007. 2007. • 43. British HIV Association. Clinical Audit Report 2010-11. 2011. • 44. British HIV Association. BHIVA guidelines for the treatment of HIV-1 positive adults with antiretroviral therapy 2012. In Press. 2012. • 45. Lucas SB, Curtis H, Johnson MA. National Review of Deaths among HIV-infected adults. Clinical Medicine. 2008;8(3):250-2. • 46. Begg N, Cartwright KAV, Cohen J, Kaczmarski EB, Innes JA, Leen CLS, et al. Consensus Statement on Diagnosis, Investigation, Treatment and Prevention of Acute Bacterial Meningitis in Immunocompetent Adults. Journal of Infection. 1999;39:1-15. • 47. Michael B, Menezes B, Cunniffe J, Miller A, Kneen R, Francis G, et al. Effect of delayed lumbar punctures on the diagnosis of acute bacterial meningitis in adults. Emerg Med J. 2010;27:433-8. • 48. Health Protection Agency. UK Standards for Microbiology Investigations - Investigation of Viral Encephalitis and Meningitis. 2011:1-29. • Viral Meningitis • Learning Objectives • Overview • Causes of aseptic meningitis • Epidemiology • Clinical Features • Investigations • Lumbar puncture • Blood tests • Viral meningitis vs encephalitis • Treatment • Enteroviral meningitis • Herpes meningitis • VSV meningitis • HIV infection • Complications • Key points • Summary • Clinical scenarios • Self assessment
Clinical Scenario 1 You are called to see an 18 year old man in the emergency department. He has a headache, photophobia and a sore throat. He has been unwell for just over 24 hours. On examination, he is alert and talking to you, although he has difficulty keeping his eyes open. He has no signs of focal neurological weakness and he has not had any seizures. His temperature is 39.0 °C. The rest of his examination is normal and his blood tests are all within the normal range. You have already sent blood cultures. • Viral Meningitis • Learning Objectives • Overview • Causes of aseptic meningitis • Epidemiology • Clinical Features • Investigations • Lumbar puncture • Blood tests • Viral meningitis vs encephalitis • Treatment • Enteroviral meningitis • Herpes meningitis • VSV meningitis • HIV infection • Complications • Key points • Summary • Clinical scenarios • Self assessment What should you do now? CT scan Lumbar Puncture MRI brain
Question 1 Answer the following question true or false • Viral Meningitis • Learning Objectives • Overview • Causes of aseptic meningitis • Epidemiology • Clinical Features • Investigations • Lumbar puncture • Blood tests • Viral meningitis vs encephalitis • Treatment • Enteroviral meningitis • Herpes meningitis • VSV meningitis • HIV infection • Complications • Key points • Summary • Clinical scenarios • Self assessment Viral meningitis is a notifiable condition in the UK? TRUE FALSE
To learn more about neurological infectious diseases… NeuroID 2013: Liverpool Neurological Infectious Diseases Course Liverpool Medical Institution, UK Provisional date: May 2013 Ever struggled with a patient with meningitis or encephalitis, and not known quite what to do? Then the Liverpool Neurological infectious Diseases Course is for you! For Trainees and Consultants in Adult and Paediatric Neurology, Infectious Diseases, Acute Medicine, Emergency Medicine and Medical Microbiology who want to update their knowledge, and improve their skills. • Presented by Leaders in the Field • Commonly Encountered Clinical Problems • Practical Management Approaches • Rarities for Reference • Interactive Case Presentations • State of the Art Updates • Pitfalls to Avoid • Controversies in Neurological Infections Feedback from previous course: “Would unreservedly recommend to others” “An excellent 2 days!! The best course for a long time” Convenors: Prof Tom Solomon, Dr EnitanCarrol, Dr Rachel Kneen, Dr Nick Beeching, Dr Benedict Michael For more information and to REGISTER NOW VISIT: www.liv.ac.uk/neuroidcourse