Download
1 / 42
420 likes | 537 Views
MSMA HIT for the Physician January 30, 2010. Karen Edison, MD Center for Health Policy University of Missouri, Columbia. “Information is the lifeblood of modern medicine. Health information technology (HIT) is destined to be its circulatory system.”. David Blumenthal, M.D., M.P.P.

E N D
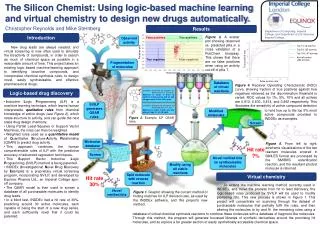
MSMAHIT for the PhysicianJanuary 30, 2010 Karen Edison, MD Center for Health Policy University of Missouri, Columbia
“Information is the lifeblood of modern medicine. Health information technology (HIT) is destined to be its circulatory system.” David Blumenthal, M.D., M.P.P.
HITECH Act – Health Information Technology for Economic and Clinical Health Part ($2B) of the American Recovery and Reinvestment Act of 2009 aka “ARRA” or the “Stimulus Bill”
New programs • Regional Centers $673 M • HI exchange - states $564 M • Workforce training $118 M • Beacon communities $235 M • HIT research (SHARP) $60 M • NHIN (National HI network) & • Standards and certification $64 M
New Regulations – open for comment! • Meaningful use • Certification
Background Information • CMS released notice of proposed rulemaking on “meaningful use” of certified electronic health records on Dec. 30, 2009 • The Office of the National Coordinator for Health Information Technology (ONC) released its complementary certification standards • Both rules published in Federal Register January 13, 2010. • ONC: interim final rule; effective date February 12, 2010, but changes are still possible. • Comments are strongly encouraged: Deadline March 15, 2010. Source: Association of American Medical Colleges & Manatt Health Solutions
“Meaningful Use” • Using EHR technology in a meaningful manner. • Requires meaningful use measures to become more stringent over time. Source: Association of American Medical Colleges
Proposed Stages of Meaningful Use By Payment Year Source: Association of American Medical Colleges
Medicare and Medicaid Rules EPs (eligible professionals) choose between Medicare & Medicaid (must be 30% of pts. except for peds who need 20%) Medicare and Medicaid rules: mostly consistent One-time switch no later than 2014 Source: Association of American Medical Colleges
Incentives for Eligible Professionals • Medicare payments are available for EPs that are paid under the physician fee schedule (PFS) • Medicare payments will be determined on an individual-practitioner basis • Each year under the EHR Incentive Program, an EP will receive 75 percent of the EP’s total “allowed charges” during the Payment Year, subject to a cap. • The payment limit for the first year depends on when the EP begins “meaningful use” of an EHR system. Source: Manatt Health Solutions
3 Stages of Objectives • Stage 1: (details in this proposed rule) • Using information to track key clinical conditions and communicating that information for care coordination • Implementing clinical decision support tools • Reporting clinical quality measures and public health information Source: Association of American Medical Colleges
Stage 2:(Proposed by end of 2011) • Expand stage 1 criteria to encourage using health IT for quality improvement • Exchange of information in most structured format possible Source: Association of American Medical Colleges
Stage 3: (Proposed by end of 2013) • Promote improvements in quality, safety, and efficiency • Decision support for national high priority conditions • Patient access to self-management tools • Access to comprehensive patient data • Improving population health
Stage 1 Highlights 25 measures corresponding to Stage 1 objectives for EPs Must meet all 25 measures Yes/No Measures Source: Association of American Medical Colleges
Baseline Requirement 50% or more of patent encounters during the reporting period at practice(s)/location(s) equipped with certified EHR technology Source: Association of American Medical Colleges
Examples of Yes/No Measures Implement drug-drug, drug-allergy, drug-formulary checks Generated at least 1 report of patients with specific condition Implement 5 clinical decision support rules One test of electronic exchange of key clinical information Source: Association of American Medical Colleges
Examples of Yes/No Measures One test of electronic data submission to immunization registry One test of electronic syndromic surveillance data to public health agency Conduct or review security risk analysis and implement security updates Source: Association of American Medical Colleges
Measures requiring a numerator and denominator • Higher % for criteria based on capability • Lower % if electronic exchange of information
Stage 1 Highlights 25 measures corresponding to Stage 1 objectives for EPs Must meet all 25 measures Yes/No Measures Source: Association of American Medical Colleges
Examples of Measures Requiring a Numerator and Denominator 75% of all permissible prescriptions transmitted electronically 10% of all unique patients provided timely electronic access to their health information 80% of all unique patients have at least one medication entry (or an indication of “none”) recorded as structured data Source: Association of American Medical Colleges & Manatt Health Solutions
Examples of Measures Requiring a Numerator and Denominator 80% of all unique patients over age 12 have smoking status recorded Reminder sent to 50% of all unique patients that are age 50 or older 50% of clinical lab test ordered are incorporated in EHR technology Source: Manatt Health Solutions
Medicare Meaningful Use Reporting • How to report? Attestation through secure mechanism • 90 Day Reporting Periods for EPs • Earliest: Jan. 1, 2011-Apr. 1, 2011 • Latest: Oct. 1, 2011-Dec. 31, 2011 • Quality Reporting • 2011: Calculate and attest to results • 2012: Submit data through EHR Source: Association of American Medical Colleges
Incentive Payments • Rolling payments-90 days first year; full calendar year thereafter • Fee schedule reductions for EPs who do not achieve meaningful use: • 2015: 1% • 2016: 2% • 2017 and after: 3% • Exceptions for hardship on case-by-case basis for EPs practicing in rural areas with insufficient internet access and for hospital-based EPs Source: Association of American Medical Colleges
This is a very fluid process Your voice matters!
State activity so far………. • Establish MO-HITECH • Establish Advisory Board • Convene Workgroups • Publish Draft Strategic Plan for Review • Engage and educate stakeholders
Current state activity and plan • Convene Advisory Board & Workgroups • Publish Draft Operational Plan for Review – mid March • Engage and educate stakeholders • Submit Operational Plan – late April
MO-HITECH Advisory Board • Co-Chairs – Ronald Levy, Director DSS & HIT Coordinator and Barrett Toan • Staff – George Oestreich, Charlotte Krebs & Manatt Team: Bill Bernstein, Melinda Dutton, Tim Andrews, Kier Wallis • Membership – 18 people from public and private sector
Physician members of the Advisory Board • Karen Edison, MD, Center for Health Policy • Tracy Godfrey, MD, Family Physician, Joplin • Ian McCaslin, MD, MO HealthNet Director • Tom Hale, MD, PhD, Sisters of Mercy, St. Louis
Workgroups • Governance • Finance • Technical Infrastructure • Business and Technical Operations • Legal/Policy • Consumer Engagement
Missouri Health Information Technology (HIT) Assistance Center
Core Applicant Team • University of Missouri’s • Health Management and Informatics (HMI) Department • Center for Health Policy (CHP) • Missouri Telehealth Network (MTN) • Family and Community Medicine (FCM) Department
Key Partners • Primaris (Missouri’s Quality Improvement Organization) • Missouri Primary Care Association (MPCA) • Kansas City Quality Improvement Collaborative (KCQIC)
Mission • To help primary care providers and others to • Choose an EHR • Re-engineer office workflow • Implement an EHR and deal with vendors • Achieve “meaningful use” • Pull down incentives
“Knowing is not enough; we must apply.Willing is not enough; we must do.”—Goethe
If you are interested in the State HIE processwww.dss.mo.gov/hieIf you are interested in the services of the Missouri HIT Assistance Center Hoytav@health.Missouri.edu