Download

1 / 55
550 likes | 831 Views
Neurobehavioral Patterns Across the Spectrum in FASD. Dr. Ana Hanlon-Dearman Developmental Pediatrician Clinic for Alcohol and Drug Exposed Children Assistant Professor Pediatrics and Child Health University of Manitoba Winnipeg, MB. Goals of Session:.

E N D
Neurobehavioral Patterns Across the Spectrum in FASD Dr. Ana Hanlon-Dearman Developmental Pediatrician Clinic for Alcohol and Drug Exposed Children Assistant Professor Pediatrics and Child Health University of Manitoba Winnipeg, MB Clinic for Alcohol and Drug Exposed Children
Goals of Session: • Brain:To review current research on anatomic and neurotransmitter correlates of brain function • Behavior:To describe at neurodevelopmental correlates of brain function in FASD • Across the spectrum • Over time • Promising questions for future research Clinic for Alcohol and Drug Exposed Children
Brain in FASD • Integration of molecular, cellular, chemical, anatomic, and behavioral research Clinic for Alcohol and Drug Exposed Children
Brain plasticity and neurodevelopment • Traditionally: • fixed number of adult neurons • synaptogenesis • neurotransmitter functions (receptors, release of neurochemicals) http://www.utexas.edu/research/asrec/synapse_m.html Clinic for Alcohol and Drug Exposed Children
Novel processes of neuronal development Neural Stem cells Mood Neurogenesis Learning Sensory Processing Behavior Memory Clinic for Alcohol and Drug Exposed Children
Alcohol and neuronal development • Does alcohol exposure affect neuronal development? • Could this damage be repaired? Clinic for Alcohol and Drug Exposed Children
Alcohol and regulation of neurogenesis • Genetics influences responses to alcohol • Environment affects plasticity Alcohol Genetics Alcohol Stress Environment Clinic for Alcohol and Drug Exposed Children
Physiology and Function Cognitive Function Sensory regulation Neurotransmitters Growth Factors ?Circadian regulation Motor function Clinic for Alcohol and Drug Exposed Children
What does that mean over the spectrum? • Fetal neural stem cells are highly susceptible to alcohol toxicity (Luo and Miller. 1998) • Alcohol affects neurogenesis in high doses, as well as moderate chronic doses Clinic for Alcohol and Drug Exposed Children
With this in mind… • Discuss our clinical research into • specific manifestations of alcohol toxicity on learning structures and their function • alcohol effects on circadian rhythm and sleep • neurodevelopmental functions over time Clinic for Alcohol and Drug Exposed Children
FASD FAS pFAS ARND What is the neurodevelopmental spectrum of alcohol effects? • Language • Executive function • Attention • Memory • Visual spatial skills • Motor coordination • Cognitive processing Clinic for Alcohol and Drug Exposed Children
Attention Sensorimotor Structural malformation Executive Function Language Memory Cognitive Function Academic Achievement Adaptive Clinic for Alcohol and Drug Exposed Children
Some of our questions… • Can we define specific learning impairments? • Can we define specific sensory impairments? • What about ARND? • What happens over time? Clinic for Alcohol and Drug Exposed Children
Learning… Clinic for Alcohol and Drug Exposed Children
encoding Working Memory retrieval retaining Central Executive Visual + spatial Phonological Episodic buffer Clinic for Alcohol and Drug Exposed Children
14 children with FASD: FAS n=3 pFAS n=6 ARND n=5 10 adults with FASD: FAS n=3 pFAS n=1 ARND n=6 N-back test Self-ordered pointing task (SOPT) Continuous Performance Test Wisconsin Card Sorting Task Participants Methods Clinic for Alcohol and Drug Exposed Children
N back task N=0 N=1 N=2 Clinic for Alcohol and Drug Exposed Children
Results: Mean scores in each n-back task Clinic for Alcohol and Drug Exposed Children
Results: 1 Back minus Simple -- 11 year old children FAS pFAS Control Clinic for Alcohol and Drug Exposed Children
FASD: Increased functional activation in inferior-middle frontal and orbital gyrus Greater activation in cingulate cortex in inferior slices Decreased frontal lobe activity with increasing task difficulty Controls: Greater activation in cingulate and frontal areas in superior slices Greater parietal activity Increased frontal lobe activity with increasing task difficulty Results: 11 year old children Clinic for Alcohol and Drug Exposed Children
Results: One Back minus Simple Task 26 y ARND 25 y FAS 26 y Control Clinic for Alcohol and Drug Exposed Children
Results: Adults • Adults with FASD showed greater orbital and inferior-middle frontal activation during blank test • In general, trend toward greater brain activity with increased task difficulty • Greater parietal and frontal activations with increasing task difficulty in both FASD and control (FASD<control) • Pattern less consistent in adults Clinic for Alcohol and Drug Exposed Children
Conclusions: • FASD: • dysfunction in prefrontal areas • ?decreased parietal function relative to controls(link to accuracy and effort) • Activation in cingulate(link to affective behaviors, executive function) • Impairment in spatial working memory • Independent of cognitive and response inhibition Clinic for Alcohol and Drug Exposed Children
Sensory…. Clinic for Alcohol and Drug Exposed Children
Sleep Characteristics of Young Alcohol Affected Children: A Quantitative and Qualitative StudyA. Hanlon-Dearman, CADEC Team Clinic for Alcohol and Drug Exposed Children
I used to hear him constantly, just moving all the time…he would mumble and whine or whatever but nothing that I could make out. That’s if he wasn’t waking up crying or screaming…anywhere from once to two to three times per night. (Interview #1) Clinic for Alcohol and Drug Exposed Children
Methods: • N=9 children • household matched controls • Tools: • actigraphy and sleep log • sleep questionnaire • interviews Clinic for Alcohol and Drug Exposed Children
Actigraphy results:repeated measures ANOVA FASD vs Controls Clinic for Alcohol and Drug Exposed Children
Questionnaire results • FASD sleep related concernsOR 35.29 (p=0.009) • Talking (44%) • Difficulty settling (33%) • Daytime fatigue (11%) • Nightime wakenings: 23 times more likely to wake related to own movements (OR 23.22 p=0.0294) • Daytime behavior concerns: hyperactivity OR 3.0 (p=0.009) Clinic for Alcohol and Drug Exposed Children
Conclusions • First objective study of sleep characteristics in FASD children • Confirms significantly disrupted nighttime sleep • Increased frequency and length of night wakenings • Parental report of concerns re: sleep is significantly greater than those related to hyperactivity Clinic for Alcohol and Drug Exposed Children
He needed to be bundled for quite a long time…We have these sort of rough, massaging type of gloves that we rub him down with, and he really likes that with some gel. Before this, he gets a bath with a calming lavender bath from the States…Then we do the rub down with the gloves, and he really likes that. Then, we go into the rocking chair and we rock him for about 15-20 minutes. Then, we go up to his room where we read him a story, and then he knows he has to lie down or play quietly. (Interview #4) Clinic for Alcohol and Drug Exposed Children
Sleep and Sensory Processing in Young Children (0-36 months) with FASD -- A pilot studyA. Hanlon-Dearman, B. Fjeldsted, CADEC Team Clinic for Alcohol and Drug Exposed Children
Alcohol teratogenicity Neurotransmitters Sensory Processing Sleep Clinic for Alcohol and Drug Exposed Children
Methods • N=20 children with FASD Tools used: • Infant/Toddler Sensory Profile (Dunn and Daniels, The Psychological Corporation, 2002) • Brief Infant Sleep Questionnaire (BISQ) developed by Sadeh (2004) Clinic for Alcohol and Drug Exposed Children
Results: • Significant Correlations : • total daytime sleep and sensation seeking (raw) rs=-0.56 (p=0.0103) • pm wakefulness and sensation avoiding rs=0.46 (p=0.0421) • pm wakefulness and oral (raw) rs=-0.44 (p=0.0494) Clinic for Alcohol and Drug Exposed Children
Conclusions • First study to correlate sleep dysfunction with sensory processing abnormalities in FASD • Sensory processing abnormalities correlated with both daytime and nighttime dysfunction Clinic for Alcohol and Drug Exposed Children
Neurodevelopmental patterns over time… Clinic for Alcohol and Drug Exposed Children
Background • 20 years of longitudinal studies have shown persistent behavioral, learning, and adaptive difficulties into adulthood(Spohr, 2007; Autti-Ramo, 2000; Spohr, 1993; Streissguth, 1991) • Deficits in social/adaptive behavior may become more significant with age(Whaley et al. 2001) Clinic for Alcohol and Drug Exposed Children
Factors influencing outcomes Family Dose Individual factors Alcohol Environment School Timing Community Clinic for Alcohol and Drug Exposed Children
Age related Neurodevelopmental Abnormalities in Children with pFAS and ARNDS. Longstaffe, A. Hanlon-Dearman, K. Penner, and CADEC Team Clinic for Alcohol and Drug Exposed Children
Method • Retrospective analysis of clinical data • N=60 • Children were grouped into 2 categories: • 6-9 years (n=32) • 10 - 12 years (n=28). Clinic for Alcohol and Drug Exposed Children
Assessment Tool NEPSY: A neuropsychological assessment tool for children ages 3-12 • 27 subtests assessing 5 domains: Attention/Executive Function, Language, Sensorimotor, Visuospatial, Memory and Learning • Qualitative analysis of motor function, error patterns and critically significant core domain discrepancies Clinic for Alcohol and Drug Exposed Children
Male 11.8 yrs presents with history of increasing school failure, externalizing, internalizing, & ADHD problem behaviors. Nondysmorphic, well grown In group home following family and multiple placement breakdowns. Artistic, qualitative motor concerns, “doesn’t listen”. Final Dx: ARND A NEPSY PROFILE Clinic for Alcohol and Drug Exposed Children
Results: Clinic for Alcohol and Drug Exposed Children
Auditory vs Visual:Attention and Memory Clinic for Alcohol and Drug Exposed Children
Frequency of Significant Domain Discrepancies Clinic for Alcohol and Drug Exposed Children
Visual spatial domain a consistent strength • Attention/executive function, language and memory core domains were globally significant weaknesses • N=54, p<0.05 Clinic for Alcohol and Drug Exposed Children
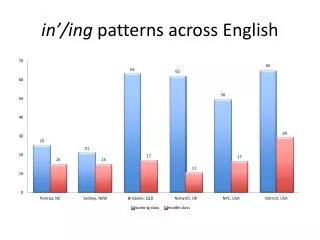
Error patterns • Increasing disorganization and difficulty processing complex auditory, but not visual information Clinic for Alcohol and Drug Exposed Children
Conclusions • Changes in NEPSY scores occur over time • Specific deficits in language, memory and attention, at various age groups • Refining the Canadian Diagnostic Guidelines may be needed to consider possible differential expression of core deficits over time Clinic for Alcohol and Drug Exposed Children