Download
1 / 1
20 likes | 181 Views
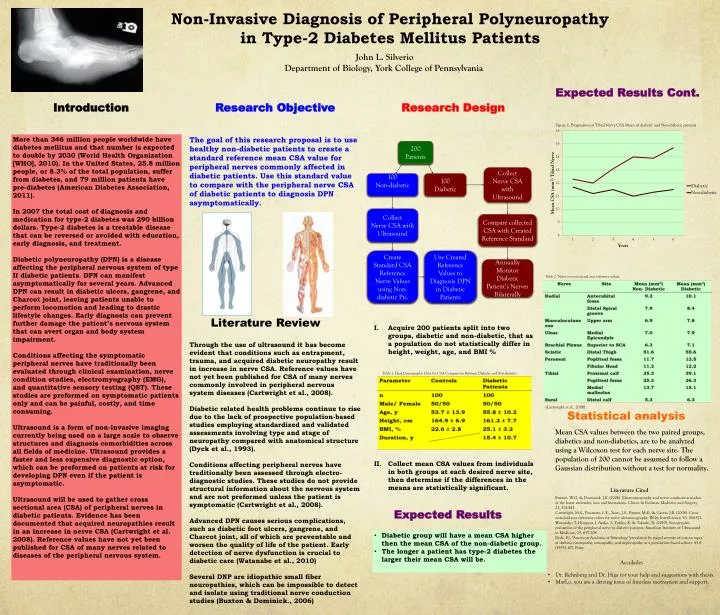
Non-Invasive Diagnosis of Peripheral Polyneuropathy in Type-2 Diabetes Mellitus Patients. 200 Patients. Figure 1. Progression of Tibial Nerve CSA Mean of diabetic and Non-diabetic patients. Collect Nerve CSA with Ultrasound. 100 Non-diabetic. 100 D iabetic.

E N D
Non-Invasive Diagnosis of Peripheral Polyneuropathy in Type-2 Diabetes Mellitus Patients 200 Patients Figure 1. Progression of Tibial Nerve CSA Mean of diabetic and Non-diabetic patients Collect NerveCSA with Ultrasound 100 Non-diabetic 100 Diabetic John L. Silverio Department of Biology, York College of Pennsylvania Collect NerveCSA with Ultrasound Compare collected CSA with Created Reference Standard Create Standard CSA Reference Nerve Values using Non-diabetic Pts. Use Created Reference Values to Diagnosis DPN in Diabetic Patients Annually Monitor Diabetic Patient’s Nerves Bilaterally Expected Results Cont. Introduction Research Objective Research Design More than 346 million people worldwide have diabetes mellitus and that number is expected to double by 2030 (World Health Organization [WHO], 2010). In the United States, 25.8 million people, or 8.3% of the total population, suffer from diabetes, and 79 million patients have pre-diabetes (American Diabetes Association, 2011). In 2007 the total cost of diagnosis and medication for type-2 diabetes was 290 billion dollars. Type-2 diabetes is a treatable disease that can be reversed or avoided with education, early diagnosis, and treatment. Diabetic polyneuropathy (DPN) is a disease affecting the peripheral nervous system of type II diabetic patients. DPN can manifest asymptomatically for several years. Advanced DPN can result in diabetic ulcers, gangrene, and Charcot joint, leaving patients unable to perform locomotion and leading to drastic lifestyle changes. Early diagnosis can prevent further damage the patient’s nervous system that can avert organ and body system impairment. Conditions affecting the symptomatic peripheral nerves have traditionally been evaluated through clinical examination, nerve condition studies, electromyography (EMG), and quantitative sensory testing (QST). These studies are preformed on symptomatic patients only and can be painful, costly, and time consuming. Ultrasound is a form of non-invasive imaging currently being used on a large scale to observe structures and diagnosis comorbidities across all fields of medicine. Ultrasound provides a faster and less expensive diagnostic option, which can be preformed on patients at risk for developing DPN even if the patient is asymptomatic. Ultrasound will be used to gather cross sectional area (CSA) of peripheral nerves in diabetic patients. Evidence has been documented that acquired neuropathies result in an increase in nerve CSA (Cartwright et al. 2008). Reference values have not yet been published for CSA of many nerves related to diseases of the peripheral nervous system. The goal of this research proposal is to use healthy non-diabetic patients to create a standard reference mean CSA value for peripheral nerves commonly affected in diabetic patients. Use this standard value to compare with the peripheral nerve CSA of diabetic patients to diagnosis DPN asymptomatically. Literature Review • Acquire 200 patients split into two groups, diabetic and non-diabetic, that as a population do not statistically differ in height, weight, age, and BMI % • Collect mean CSA values from individuals in both groups at each desired nerve site, then determine if the differences in the means are statistically significant. Through the use of ultrasound it has become evident that conditions such as entrapment, trauma, and acquired diabetic neuropathy result in increase in nerve CSA. Reference values have not yet been published for CSA of many nerves commonly involved in peripheral nervous system diseases (Cartwright et al., 2008). Diabetic related health problems continue to rise due to the lack of prospective population-based studies employing standardized and validated assessments involving type and stage of neuropathy compared with anatomical structure (Dyck et al., 1993). Conditions affecting peripheral nerves have traditionally been assessed through electro-diagnostic studies. These studies do not provide structural information about the nervous system and are not preformed unless the patient is symptomatic (Cartwright et al., 2008). Advanced DPN causes serious complications, such as diabetic foot ulcers, gangrene, and Charcot joint, all of which are preventable and worsen the quality of life of the patient. Early detection of nerve dysfunction is crucial to diabetic care (Watanabe et al., 2010) Several DNP are idiopathic small fiber neuropathies, which can be impossible to detect and isolate using traditional nerve conduction studies (Buxton & Dominick., 2006) Table 1. Ideal Demographic Data for CSA Comparison Between Diabetic and Non-diabetic Statistical analysis Table 2. Nerve cross-sectional area reference values. Mean CSA values between the two paired groups, diabetics and non-diabetics, are to be analyzed using a Wilcoxon test for each nerve site. The population of 200 cannotbeassumed to follow a Gaussian distribution without a test for normality. Literature Cited Buxton, W.G, & Dominick, J.E. (2006). Electromyography and nerve conduction studies of the lower extremity: uses and limitations. Clinics In Podiatric Medicine and Surgery, 23, 531-543. Cartwright, M.S., Passmore, L.E., Yoon, J.S., Brown, M.E., & Caress, J.B. (2008). Cross-sectional area reference values for nerve ultrasonography. Wiley InterScience, 10, 566-571. Watanabe, T, Hiroyasu, I, Ayako, S, Yuriko, K, & Takashi, N. (2010). Sonographic evaluation of the peripheral nerve in diabetic patients. American Institute of Ultrasound in Medicine, 29, 697-708. Dyck, P.J. "American Academy of Neurology."prevalence by staged severity of various types of diabetic neuropathy, retinopathy, and nephropathy in a population‐based cohort. 43.4 (1993): 817. Print. Expected Results (Cartwright et al., 2008) • Diabetic group will have a mean CSA higher then the mean CSA of the non-diabetic group. • The longer a patient has type-2 diabetes the larger their mean CSA will be. Accolades • Dr. Rehnberg and Dr. Higa for your help and suggestions with thesis. • MarLo, you are a driving force of limitless motivation and support.