Download
1 / 32
330 likes | 544 Views
Testosterone Effect on Lipids ,Bone Density and Breast Cancer Incidence. The “ABC Study”. This is a preliminary view of data collected on women receiving testosterone with oestrogen replacement in the menopause These data are yet to be finally analysed.

E N D
Testosterone EffectonLipids ,Bone Densityand Breast Cancer Incidence The “ABC Study”
This is a preliminary view of data collected on women receiving testosterone with oestrogen replacement in the menopauseThese data are yet to be finally analysed.
A retrospective data collection was undertaken.A list of patients receiving testosterone were drawn from the computer billing record and contacted by telephone.The interview was conducted by a research assistant with a standardised questionnaire.
520 women received testosterone and oestrogen by implant over 12 years.The current population of women receiving both testosterone and oestrogen in my practice at that time was:1000+/- patients
Oestrogen was given at 5-12 month intervals.Testosterone was given at 5-6 monthly intervals. The dose of testosterone varied between 50 and 100 mgm and rarely 150 mgm.
The dose of implant was selected on subjective response, checked by objective measurement and reduced if adverse side effects emerged.
The measured total level would often exceed the premenopausal “normal range”.The relevant level would be the bioavailable range(testosterone / SHBG“testosterone index”).
Originally the testosterone was used in line with conventional medical wisdom to improve libido.Quite quickly it became apparent that this was not the major benefit that the hormone could confer on the woman.
The data included in addition to basic clinical information, • benign breast disease • breast cancer • HDL/ LDL • hip and spine density
Total no. attempted contact 536Successful contact 520Unable to contact 11Gone o/s or i/s 5
Women receiving oestrogen replacement in the menopause have been given the expectation that it will give a cardioprotective effect at least in terms of the proxy markers of HDL and LDL cholesterol.
It would be of concern if that protective effect was lost with the introduction of testosterone.HDL and LDL were followed over the 12 year span.
HDL Cholesterol S.D. 0.3-0.5
LDL Cholesterol SD 0.9-1.1
It would appear that there was no serious adverse effect by the testosterone on these two markers.The mean levels while varying over time, would be acceptable.
The addition of testosterone to conventional HRT has the reputation for improving bone density.This assertion was examined.
Change in Lumbar Density Range 0.77-1.60 +3.1%
Change in Hip Density Range 0.77-1.37 +3.1%
Change in LS BMD over 3 years 8 6 Series1 4 % Change in BMD 2 0 LS1 LS2 LS3 BMD YEARS
The initial improvement in bone density of only 3.1% in either area fell short of expectation as did the overall loss.Declining densities in smaller numbers was attributed to non- responders to HRT.
As the years passed, it was noted that the testosterone appeared to have the capacity to reduce oestrogen stimulated breast soreness and the incidence of abnormal mammograms appeared to be reduced.
The only possible exception to this would be when the woman was inadequately replaced with oestrogen.Under these circumstances it is believed that there may have been increased aromatisation of testosterone to oestrogen within the breast tissue
The simplistic idea emerged that if oestrogen was at least a promoter of breast cancer, and if testosterone reduced breast stimulation, might it not be shown to decrease the incidence of breast cancer?
A survival analysis for the study group was undertaken.The starting date for the measurement of survival time was the date of first testosterone implant.The end time was the date of last follow up for those women not diagnosed with breast cancer, and date of diagnosis for those women diagnosed with breast cancer.
The survival time was compared with data taken from the S. A. Cancer Registry.
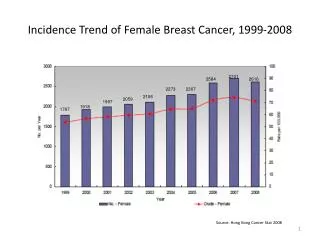
The 10-year breast cancer free survival rate for patients in the trial was 97.41%. (95% confidence interval of 95.53% to 99.29%.) The expected 10-year breast cancer free survival rate for patients in the trial was 97.52%.
It would appear then that the survival from the diagnosis breast cancer did not differ from that of the South Australian population at large of whom 44.3% were taking oestrogens.
It would have been optimal to compare the study group with women taking oestrogen alone.A statistical estimate was made of expected rates if 100% of the women in the Omnibus Study had been taking oestrogen.The R.R. of 1.35 (Beral et al) was used in this exercise.
The S. A. Health Omnibus Study tells us that in 1997 the current use of oestrogen was a maximum of 44.3% and the ‘ever use’ was 63.6%, and that only 5.4% of these had ever used testosterone.
The calculation shows that the expected 10-year breast cancer free survival rate for patients in the trial was ?? 92% vs. 97.41%. (95% confidence interval of 95.53% to 99.29%.) It might therefore be suspected that if the testosterone users were compared with oestrogen only users, the incidence of breast cancer would be reduced.