Download
1 / 145
1.55k likes | 2.35k Views
Anthrax. Anthrax: History. Caused by Bacillus anthracis Human zoonotic disease Spores found in soil worldwide Primarily disease of herbivorous animals Sheep, goats, cattle Many large documented epizootics Occasional human disease Epidemics have occurred but uncommon

E N D
Anthrax: History • Caused by Bacillus anthracis • Human zoonotic disease • Spores found in soil worldwide • Primarily disease of herbivorous animals • Sheep, goats, cattle • Many large documented epizootics • Occasional human disease • Epidemics have occurred but uncommon • Rare in developed world Saint Louis Unversity School of Public Health
Anthrax: Bioweapon Potential • Many countries have weaponized anthrax • Former bioweapon programs • U.S.S.R.,U.S.,U.K., and Japan • Recent bioweapon programs • Iraq • Attempted uses as bioterrorism agent • WW I: Germans inoculated Allied livestock • WW II: Alleged Japanese use on prisoners Saint Louis Unversity School of Public Health
Anthrax: Bioweapon Potential • Features of anthrax suitable as BT agent • Fairly easy to obtain, produce and store • Spores easily dispersed as aerosol • Moderately infectious • High mortality for inhalational (86-100%) Saint Louis Unversity School of Public Health
Anthrax: Bioweapon Potential • Aerosol method of delivery • Most likely method expected in BT attack • Would cause primarily inhalational disease • Spores reside on particles of 1-5 μm size • Optimal size for deposition into alveoli • Form of disease with highest mortality • Would infect the largest number of people Saint Louis Unversity School of Public Health
Anthrax: Bioweapon Potential • Dispersed as powder • Frequent letter hoaxes since 1997 • Recent letter deliveries • Highest risk is for cutaneous • Inhalational theoretically possible • Particle size • Likelihood of aerosolization • GI theoretically possible • Spores > hands > eating without handwashing Saint Louis Unversity School of Public Health
Anthrax: Bioweapon Potential • Sverdlovsk, Russia 1979 • Accidental release from anthrax drying plant • 79 human cases • All downwind of plant • 68 deaths • Some infected with multiples strains Saint Louis Unversity School of Public Health
Anthrax: Bioweapon Potential • Estimated effects of inhalational anthrax • 100 kg spores released over city size of Washington DC • 130,000 – 3 million deaths depending on weather conditions • Economic impact • $26.2 billion/100,000 exposed people Saint Louis Unversity School of Public Health
Anthrax: Epidemiology • Three forms of natural disease • Inhalational • Rare (<5%) • Most likely encountered in bioterrorism event • Cutaneous • Most common (95%) • Direct contact of spores on skin • Gastrointestinal • Rare (<5%), never reported in U.S. • Ingestion Saint Louis Unversity School of Public Health
Anthrax: Epidemiology • All ages and genders affected • Occurs worldwide • Endemic areas - Africa, Asia • True incidence not known • World 20,000-100,000 in 1958 • U.S. 235 total reported cases 1955-1994 • 18 cases inhalational since 1900, last one 1976 • Until 2001, last previous case cutaneous 1992 Saint Louis Unversity School of Public Health
Anthrax: Epidemiology • Mortality • Inhalational 86-100% (despite treatment) • Era of crude intensive supportive care • Cutaneous <5% (treated) – 20% (untreated) • GI approaches 100% Saint Louis Unversity School of Public Health
Anthrax: Epidemiology • Incubation Period • Time from exposure to symptoms • Very variable for inhalational • 2-43 days reported • Theoretically may be up to 100 days • Delayed germination of spores Saint Louis Unversity School of Public Health
Anthrax: Epidemiology • Human cases – historical risk factors • Agricultural • Exposure to livestock • Occupational • Exposure to wool and hides • Woolsorter’s disease = inhalational anthrax • Rarely laboratory-acquired Saint Louis Unversity School of Public Health
Anthrax: Epidemiology • Transmission • No human-to-human • Naturally occurring cases • Skin exposure • Ingestion • Airborne • Bioterrorism • Aerosol (likely) • Small volume powder (possible) • Foodborne (unlikely) Saint Louis Unversity School of Public Health
Anthrax: Epidemiology • Transmission • Inhalational • Handling hides/skins of infected animals • Microbiology laboratory • Intentional aerosol release • Small volume powdered form • In letters, packages, etc • Questionable risk, probably small Saint Louis Unversity School of Public Health
Anthrax: Epidemiology • Transmission • Cutaneous • Handling hides/skins of infected animals • Bites from arthropods (very rare) • Handling powdered form in letters, etc. • Intentional aerosol release • May see some cutaneous if large-scale Saint Louis Unversity School of Public Health
Anthrax: Epidemiology • Transmission • Gastrointestinal • Ingestion of meat from infected animal • Ingestion of intentionally contaminated food • Not likely in large scale • Spores not as viable in large volumes of water • Ingestion from powder-contaminated hands • Inhalational of spores on particles >5 m • Land in oropharynx Saint Louis Unversity School of Public Health
Anthrax: Microbiology • Bacillus anthracis • Aerobic, Gram positive rod • Long (1-10μm), thin (0.5-2.5μm) • Forms inert spores when exposed to O2 • Infectious form, hardy • Approx 1μm in size • Vegetative bacillus state in vivo • Result of spore germination • Non-infectious, fragile Saint Louis Unversity School of Public Health
Anthrax: Microbiology • Colony characteristics • Large (4-5mm) • Non-hemolytic • Opaque white, gray • Retain shape when manipulated (“egg white”) • Forms capsule at 37º C, 5-20% CO2 Saint Louis Unversity School of Public Health
Anthrax: Microbiology • Classification • Same family: B. cereus, B. thuringiensis • Differentiation from other Bacillus species • Non-motile • Non β-hemolytic on blood agar • Does not ferment salicin • Note: Gram positive rods are usually labeled as “contaminants” by micro labs Saint Louis Unversity School of Public Health
Anthrax: Microbiology • Environmental Survival • Spores are hardy • Resistant to drying, boiling <10 minutes • Survive for years in soil • Still viable for decades in perma-frost • Favorable soil factors for spore viability • High moisture • Organic content • Alkaline pH • High calcium concentration Saint Louis Unversity School of Public Health
Microbiology • Virulence Factors • All necessary for full virulence • Two plasmids • Capsule (plasmid pXO2) • Antiphagocytic • 3 Exotoxin components (plasmid pXO1) • Protective Antigen • Edema Factor • Lethal Factor Saint Louis Unversity School of Public Health
Anthrax: Microbiology • Protective Antigen • Binds Edema Factor to form Edema Toxin • Facilitates entry of Edema Toxin into cells • Edema Factor • Massive edema by increasing intracellular cAMP • Also inhibits neutrophil function • Lethal Factor • Stimulates macrophage release of TNF-α, IL-1β • Initiates cascade of events leading to sepsis Saint Louis Unversity School of Public Health
Anthrax: Pathogenesis • Disease requires entry of spores into body • Exposure does not always cause disease • Inoculation dose • Route of entry • Host immune status • May depend on pathogen strain characteristics Saint Louis Unversity School of Public Health
Anthrax: Pathogenesis • Forms of natural disease • Inhalational • Cutaneous • Gastrointestinal • Determined by route of entry • Disease occurs wherever spores germinate Saint Louis Unversity School of Public Health
Anthrax: Pathogenesis • Inhalational • Spores on particles 1-5 m • Inhaled and deposited into alveoli • Estimated LD50 = 2500 – 55,000 spores • Dose required for lethal infection in 50% exposed • Contained in imperceptibly small volume Saint Louis Unversity School of Public Health
Anthrax: Pathogenesis • Inhalational • Phagocytosed by alveolar macrophages • Migration to mediastinal/hilar lymph nodes • Germination into vegetative bacilli • Triggered by nutrient-rich environment • May be delayed up to 60 days • Factors not completely understood • Dose, host factors likely play a role • Antibiotic exposure may contribute • Delayed germination after antibiotic suppression Saint Louis Unversity School of Public Health
Anthrax: Pathogenesis • Inhalational • Vegetative bacillus is the virulent phase • Active toxin production • Hemorrhagic necrotizing mediastinitis • Hallmark of inhalational anthrax • Manifests as widened mediastinum on CXR • Does NOT cause pneumonia • Followed by high-grade bacteremia • Seeding of multiple organs, including meninges Saint Louis Unversity School of Public Health
Anthrax: Pathogenesis • Inhalational • Toxin production • Has usually begun by time of early symptoms • Stimulates cascade of inflammatory mediators • Sepsis • Multiorgan failure • DIC • Eventual cause of death • Symptoms mark critical mass of bacterial burden • Usually irreversible by this time • Clearance of bacteria unhelpful as toxin-mediated • Early research on antitoxin promising Saint Louis Unversity School of Public Health
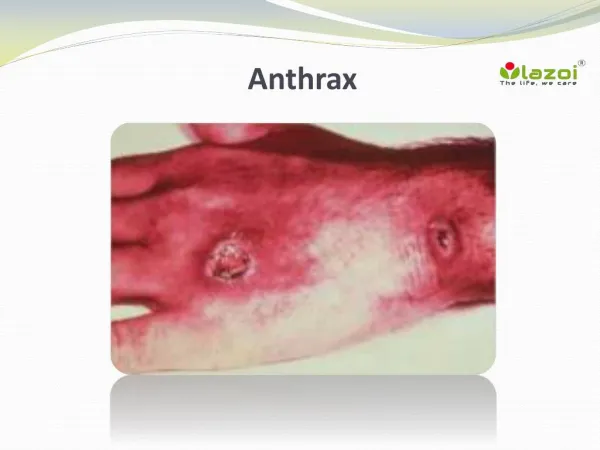
Anthrax: Pathogenesis • Cutaneous • Spores in contact with skin • Entry through visible cuts or micro-trauma • Germination in skin • Disease begins following germination • Toxin production • Local edema, erythema, necrosis, lymphocytic infiltrate • No abscess or suppurative lesions • Eventual eschar formation Saint Louis Unversity School of Public Health
Anthrax: Pathogenesis • Cutaneous • Systemic disease • Can occur, especially if untreated • Spores/bacteria carried to regional lymph nodes • Lymphangitis/lymphadenitis • Same syndrome as inhalational • Sepsis, multi-organ failure Saint Louis Unversity School of Public Health
Anthrax: Pathogenesis • Gastrointestinal • Spores contact mucosa • Oropharynx • Ingestion • Aerosolized particles >5 m • Intestinal mucosa – terminal ileum, cecum • Ingestion • Larger number of spores required for disease • Incubation period 2-5 days Saint Louis Unversity School of Public Health
Anthrax: Pathogenesis • Gastrointestinal • Spores migrate to lymphatics • Submucosal, mucosal lymphatic tissue • Mesenteric nodes • Germination to vegetative bacilli • Toxin production • Massive mucosal edema • Mucosal ulcers, necrosis • Death from perforation or systemic disease Saint Louis Unversity School of Public Health
Anthrax: Clinical Features • Symptoms depend on form of disease • Inhalational • Cutaneous • Gastrointestinal Saint Louis Unversity School of Public Health
Anthrax: Clinical Features • Inhalational • Asymptomatic incubation period • Duration 2-43 days, ~10 days in Sverdlovsk • Prodromal phase • Correlates with germination, toxin production • Nonspecific flu-like symptoms • Fever, malaise, myalgias • Dyspnea, nonproductive cough, mild chest discomfort • Duration several hours to ~3 days • Can have transient resolution before next phase Saint Louis Unversity School of Public Health
Anthrax: Clinical Features • Inhalational • Fulminant Phase • Correlates with high-grade bacteremia/toxemia • Critically Ill • Fever, diaphoresis • Respiratory distress/failure, cyanosis • Septic shock, multi-organ failure, DIC • 50% develop hemorrhagic meningitis • Headache, meningismus, delirium, coma • May be most prominent finding • Usually progresses to death in <36 hrs • Mean time from symptom onset to death ~3 days Saint Louis Unversity School of Public Health
Anthrax: Clinical Features • Laboratory Findings • Gram positive bacilli in direct blood smear • Electrolyte imbalances common • Radiographic Findings • Widened mediastinum • Minimal or no infiltrates • Can appear during prodrome phase Saint Louis Unversity School of Public Health
Anthrax: Clinical Features • Cutaneous • Most common areas of exposure • Hands/arms • Neck/head • Incubation period • 3-5 days typical • 12 days maximum Saint Louis Unversity School of Public Health
Anthrax: Clinical Features • Cutaneous – progression of painless lesions Papule – pruritic Vesicle/bulla Ulcer – contains organisms, sig. edema Eschar – black, rarely scars 24-36 hrs days Saint Louis Unversity School of Public Health
Anthrax: Clinical Features • Cutaneous • Systemic disease may develop • Lymphangitis and lymphadenopathy • If untreated, can progress to sepsis, death Saint Louis Unversity School of Public Health
Anthrax: Clinical Features • Gastrointestinal • Oropharyngeal • Oral or esophageal ulcer • Regional lymphadenopathy • Edema, ascites • Sepsis • Abdominal • Early symptoms - nausea, vomiting, malaise • Late - hematochezia, acute abdomen, ascites Saint Louis Unversity School of Public Health
Anthrax: Diagnosis • Early diagnosis is difficult • Non specific symptoms • Initially mild • No readily available rapid specific tests Saint Louis Unversity School of Public Health
Anthrax: Diagnosis • Presumptive diagnosis • History of possible exposure • Typical signs & symptoms • Rapidly progressing nonspecific illness • Widened mediastinum on CXR • Large Gram+ bacilli from specimens • Can be seen on Gram stain if hi-grade bacteremia • Appropriate colonial morphology • Necrotizing mediastinitis, meningitis at autopsy Saint Louis Unversity School of Public Health
Anthrax: Diagnosis • Definitive diagnosis • Direct culture on standard blood agar • Gold standard, widely available • Alert lab to work up Gram + bacilli if found • 6-24 hours to grow • Sensitivity depends on severity, prior antibiotic • Blood, fluid from skin lesions, pleural fluid, CSF, ascites • Sputum unlikely to be helpful (not a pneumonia) • Very high specificity if non-motile, non-hemolytic • Requires biochemical tests for >99% confirmation • Available at Reference laboratories Saint Louis Unversity School of Public Health
Anthrax: Diagnosis • Definitive diagnosis • Rapid confirmatory tests • Role is to confirm if cultures are negative • Currently available only at CDC • Polymerase Chain Reaction (PCR) • Hi sensitivity and specificity • Detects DNA • Viable bacteria/spores not required • Immunohistochemical stains • Most clinical specimens can be used Saint Louis Unversity School of Public Health
Anthrax: Diagnosis • Other diagnostic tests • Anthraxin skin test • Chemical extract of nonpathogenic B. anthracis • Subdermal injection • 82% sensitivity for cases within 3 days symptoms • 99% sensitivity 4 weeks after symptom onset • Not much experience with use in U.S. – not used Saint Louis Unversity School of Public Health
Anthrax: Diagnosis • Testing for exposure • Nasal swabs • Can detect spores prior to illness • Currently used only as epidemiologic tool • Decision for PEP based on exposure risk • May be useful for antibiotic sensitivity in exposed • Culture on standard media • Swabs of nares and facial skin • Serologies • May be useful from epidemiologic standpoint • Investigational – only available at CDC Saint Louis Unversity School of Public Health
Anthrax: Diagnosis • Environmental samples • Suspicious powders • Must be sent to reference laboratories as part of epidemiologic/criminal investigation • Assessed using cultures, stains, PCR • Air sampling • First responders • Handheld immunoassays • Not validated • Useful for detecting massive contamination Saint Louis Unversity School of Public Health
Anthrax: Diagnosis Saint Louis Unversity School of Public Health
Inhalational Influenza Pneumonia Community-acquired Atypical Pneumonic tularemia Pneumonic plague Mediastinitis Bacterial meningitis Thoracic aortic aneurysm Expect if anthrax Flu rapid diagnostic – More severe in young pts No infiltrate No prior surgery Bloody CSF with GPBs Fever Anthrax: Differential Diagnosis Saint Louis Unversity School of Public Health