Download
1 / 43
430 likes | 578 Views
Disorders of Hemostasis Resident Rounds February 5, 2004. Resident Rounds February 5, 2004. Case. 4 yo with gums that bleed for 30 mins after brushing teeth. Also had spontaneous epistaxis last week Unwell 2 weeks ago You notice petichiae around her underwear elastic ?? CBC Plt 3. ITP.

E N D
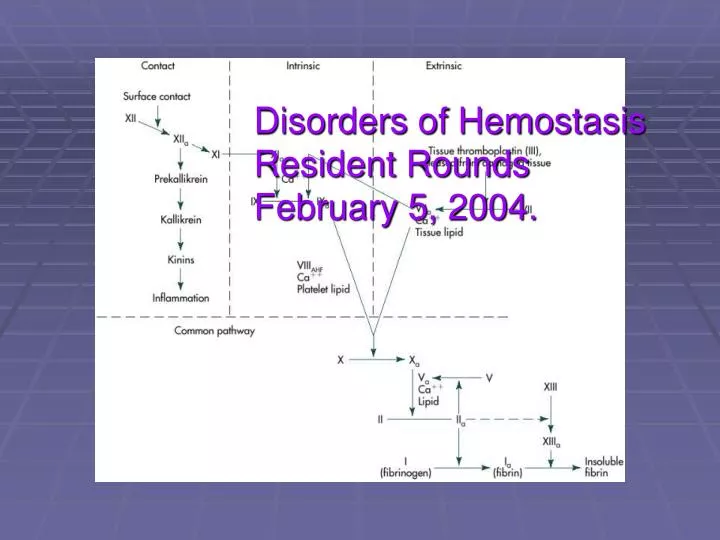
Disorders of Hemostasis Resident Rounds February 5, 2004. Resident Rounds February 5, 2004
Case • 4 yo with gums that bleed for 30 mins after brushing teeth. • Also had spontaneous epistaxis last week • Unwell 2 weeks ago • You notice petichiae around her underwear elastic • ?? • CBC • Plt 3
ITP • Children 2-6 • viral prodrome usually within 3 weeks of onset • Plts usually <20 • What do you expect their INR/PTT to be? • Bleeding time? • 90% recovery • IVIgG and steroids • splenectomy
Normal Coagulation • Depends on interaction of • Vasculature • Platelets • Coagulation cascade.
Case • 33 yo G2P1 LMP 08/05 est GA 24/40 • Presents vomiting with abdominal pain • BP 130/90, 105, 20, sats 99% • Jaundiced, tender RUQ • Labs • Hb 90, PLT 80, inc ALT/AST/bili • Coags normal • Dx??
Platelets and Coagulation Disruption of endothelial layer and exposes consituent material Platelets attach to constituent components Platelet secretion Platelet activation and aggregation
Platelet Disorders Quantitative Qualitative Decreased Production Sequestration ASA, plavix rena and hepatic disease, vWD Destruction Immune Non-immune splenomegaly TTP DIC HELLP Sepsis IPT Marrow failure
Case • 12 yo girl with menhorrhagia for 5 days • Hx of von Willebrands • Pale • HR 110, BP 90/60 • Hb 60 • Management plan?
Von Willebrand’s Disease • Defect in primary hemostasis • Quantitative (type 1 and 3) and qualitative (Type 2) • Refers to many different platelet defects • Quantitative defects of vWF most common • and mild disease is MC (approx 80%) • vWF activity reduced 20-50% normal • Most with type 1 vWF will be asymptomatic unless challenged by surgery or trauma
vWF • large multimeric glycoprotein that functions as the carrier protein for factor VIII • vWF also is required for normal platelet adhesion. As such, vWF functions in both primary (involving platelet adhesion) and secondary (involving FVIII) hemostasis. • In primary hemostasis, vWF binds on platelets to its specific receptor glycoprotein Ib and acts as an adhesive bridge between the platelets and damaged subendothelium at the site of vascular injury. • In secondary hemostasis, vWF protects FVIII from degradation and delivers it to the site of injury.
Type 1 vWF • Mild to moderate decrease in plasma levels of vWF • Proportional decrease in vWF function • Proportional decrease in circulating FVIII
Von Willebrand • Treatment options • Helpful to know • specific sub-type of disease • Previous response to currently available treatments • Immediate management depends on • Severity of disease • Type and location of bleeding
Treatment Options • DDAVP • Specific vWF and factor VIII replacement (Humate-P) • cryoprecipitate
DDAVP • Use based on observation that epi and stress increase levels of vWF and FVIII • Same effect with vasopressin and synthetic vasopressin (but no pressor effect) • Can be used IN/IV/IM (IV and IM have same effect) • 2-3X increase in vWF and FVIII • Dose = 0.2mcg/kg IV NB not effective in Type2/3 disease where pts express an abnormal ptn.
Cryoprecipitate • plasma fraction that contains factor VIII, vWF, fibrinogen, and fibronectin • obtained by harvesting the precipitate that forms when frozen plasma is warmed to 4°C. • 1 bag contains approx 100U of vWF and FVIII (approx 10x more than FFP)
Case • 12yo with hematemesis for last 6hrs • Tells you has “the worst” vonWillebrands • Type III • No detectable vWF and markedly reduced FVIII • Treatment • Cryo [+/- DDAVP]
Case • 37 yo male twisted knee and fell at work • PMHx of Hemophilia • Unsure of usual factor activity • OE tender knee hemarthrosis Do you give him factor? How much factor to give? What if you’re in High River (and you aint got none?) ?cryo
Hemophilia • A – FVIII deficiency • B – FIX deficiency • X-linked recessive • 1/3 spontaneous mutation • Mild/moderate/severe based of percent factor activity • >5%, 1-5%, <1% respectively • MC manifestations hemarthrosis and SC
Hemarthrosis • MC symptom and potentially debilitating manifestation • Spontaneous or secondary to trivial trauma • Accumulation of blood in synovial space synovial proliferation increase in joint vascularity which predisposes to further bleeding recurrent bleeding chronically deformed and painful joint
Management of Bleeding in Hemophilia • Overall principles • Depends of severity of bleeding • Underlying disease severity • Availability of replacement products • Assume during an acute bleeding episode that factor activity is 0% • Recommended to raise FVIII levels to 50%
Management of Bleeding in Hemophilia • Options • Specific factor replacement • Cryo • FFP • Do nothing
Factor replacement • 1 unit/kg of FVIII will raise plasma FVIII activity by 2% • Goal is to achieve >50% activity • Post-infusion the initial recovery of FVIII is 80% • Administer replacement at rate of 3cc/min • Peds at 100u/min • 15% will develop alloantibodies (IgG) against FVIII which neutralize exogenous administration. Pts will require 3-4X the dose of replacement.
Cryoprecipitate • Contains 100U FVIII (als contains vWF, fibrinogen, FXIII and fibronectin) • Considered a second line agent for Hem A • Dose = 2bags/10kg to raise FVIII to hemostatic levels • T ½ = 8hrs
FFP • Fluid portion of blood separated at 18C then frozen • Contains all coagulation factors • Approx 7% of of all coag factor activity of a 70kg person • Not routinely used as factor replacement in Hem A • Could consider if nothing else available
Case • 35 yo with hemophilia • Fell backwards while showing the ladies what a phat boarder he is. • No neurologic defecits • No Can CT head criteria • To the scanner? • Factor replacement if normal scan (or before scan)?
IC bleeds and the Hemophiliac • Remain a MC of death • mortality rate of 30% • Probably should receive prophylactic factor replacement • Dose of replacement • 50U/kg q12hrs • Consider cryo at 6bags/10kg
Case • 70M with likely urosepsis in ICU on pressors. • Oozing from all IV sites • INR and PTT up ? • DIC
Causes Infection GN Encapsulated GP Viruses varicella esp Massive Trauma Obstetrical Abruption Amniotic fluid embolism Malignancies Burns Transfusion-related Lab plt INR PTT FDP Fibrinogen five case studies of DIC, combining over 900 patients MC lab abn thrombocytopenia, elevated FDPs, prolonged INR, prolonged PTT, and a low fibrinogen DIC
DIC Schematic Initiation of DIC usually involves one or both of two mechanisms: mechanical tissue injury and endothelial activation and injury. Primary to both initiating pathways is the exposure of blood to huge amounts of tissue factor.
DIC • Bleeding is the predominant clinical manifestation observed in DIC • thromboembolic manifestations have been less frequently observed in DIC and have been reported in 10–40% of patients
Treat underlying stimulus Plts Maintain >30 or higher if OR planned 1U plts contained 5x109 plt expected to raise plasma by same FFP If DIC assoc with increased INR and PTT Cryo If fibrinogen <2 Give 1-4U/10kg Role for… Heparin? No established role Can worsen the situation ?consider if evidence of embolic complications in setting of DIC eg purpura fulminans ATIII -- investigational Ptn C -- investigational DICWhat to do?
Hypothermic coagulopathy • 45M found in snow bank ?duration • INR 1.6 • Plts normal • No evidence of liver failure, trauma. - EtOH • ?mechanism of coagulopathy • Likely d/t slowing of enzymatic reaction with balance favouring anti-coagulation. • Treatment? • rewarming
Case • 60 yo with ACS • Got ASA, Heparin, bblocker • Waiting for CCU • LGIB in ED • Mechanism of heparin • How do you reverse heparin?
Heparin • Unfractionated heparin • Major sites of activity ATIII, Xa • Other sites IIa, IXa, XIa • Anticoagulant effect largely through ATIII. • Produces a conformational change which accelerates the ability of ATIII to inactivate thrombin
Reversing Heparin:Protamine • T ½ = 60mins • 1mg protamine neutralizes 100 circulating units of UFH • Eg 1500U/h (no recent bolus) • 1500U + 750U + 375 = 2625U • Dose of promatime = 26.25mg • If received bolus then need to re-calculate depending on when received and add to total heparin (after 4-5hrs, bolus effectively gone)
LMWH • Inhibitor of Xa • Activity 14-16hrs • T ½ is 4hrs • Reversal is more difficult • <8hrs post-dose • 1mg protamine/1mg heparin • >8hrs • 0.5/1mg
Case • 60 with STEMI that you’ve thrombolyzed
Mechanism inducing plasmin action on fibrin contained within a thrombus T ½ 15mins Fibrinogen remains low for 24hrs Reversal Stop lytic Replenish fibrinogen Cryo FFP to correct prolonged bleeding time ?aminocarproic acid Reverse heparin Absolute lytic contraindications Hemorrhagic cerebrovascular accident, intracranial neoplasm, recent cranial surgery or trauma (10 days), uncontrolled severe hypertension Major surgery of thorax or abdomen (10 days), prolonged cardiopulmonary resuscitation, current severe bleeding (e.g., gastrointestinal) Reversing lytics
Case • 50M with known EtOH cirrhosis • Presents with abnormal coags • Pathophysiology of coagulopathy • Multiple points of insult to hemostasis: • Dec coag factor synthesis • Malabsorption/nutritional deficiency of vit. K • Portal HTN splenomegaly sequestration • Decreased synthesis of fibrinogen
Anticoagulant OD • 3 yo presents after father witnessed kid licking his lips after a mouthful of bacon and cheese rat poison 4 hrs ago. • Brings in box bromodialone 0.05% • INR normal • When would you expect it to be abnormal?
Vit. K and Coumadin • Vit K dependent coag factors? • II, VII, IX, X • Ptn C and S • Cofactor in carboxylation of enzymes which activate factors • Coumadin • T ½ = 2.5d
Supercoumadins • inhibition of the complete synthesis of the vitamin K-dependent proteins may continue for months after initial exposure, even in the absence of re-exposure. • Very high fat solubility • Can lead to prolonged INR >1yr • vitamin K1 at normal doses of administration is ineffective. • Will require daily doses of 100–150 mg of vitamin K1 administered orally have been effective in normalizing the PT. Over time, the dose of vitamin K1 needed to correct the PT can be adjusted downward, so that only the required amounts of vitamin K are employed.