Download
1 / 22
220 likes | 380 Views
Surgical Pathology Unknown Case Conference 3/26/07. Case 1: Congenital Toxoplasmosis. Congenital Toxoplasmosis. Transmission: 1° infection during gestation maternal parasitemia placental invasion ? fetal circulation

E N D
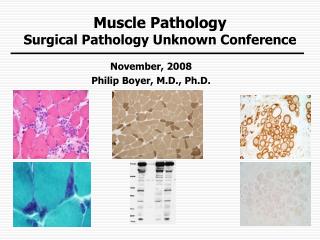
Surgical Pathology Unknown Case Conference 3/26/07 Case 1: Congenital Toxoplasmosis
Congenital Toxoplasmosis • Transmission: 1° infection during gestation maternal parasitemia placental invasion ? fetal circulation • Exceptions: reactivation (AIDS) and infection within 3 months of conception • Rate of transmission = Timing of maternal infection • Severity of disease = 1/Age of fetus at time of infection • Asymptomatic (90% infected pregnant women and 85% newborn infants) • Severe disease in antenatal/neonatal period • Asymptomatic at birth manifestations later in life • Infant with subclinical infection gestational alterations
Congenital Toxoplasmosis • Maternal diagnosis by serologic testing • Serial specimens to detect seroconversion or significant rise in IgG titer + detectable IgM • Prenatal (fetal) diagnosis by PCR of amniotic fluid and ultrasound • PCR: S=64%, NPV=88%, Sp/PPV=100% • US: ascites, hydrops, intracranial/intrahepatic calcifications, hepatosplenomegaly, hepatitis, encephalitis
Congenital Toxoplasmosis • Placental Pathology • Chronic placentitis - villitis, fibrosis, edema • TORCH: USA > 90% = CMV, T. pallidum • Large pale placenta • mild villous inflammation (histiocytes) • foci of necrotizing chronic villitis • pseudocysts in cord stroma • chronic deciduitis (nonspecific) • Granulomatous villitis
Surgical Pathology Unknown Case Conference 3/26/07 Case 2 Congenital Tuberculosis
Congenital Tuberculosis • RARE • Results from maternal tuberculous endometritis (infected AF) or miliary tuberculosis (hematogenous) • Transmitted to fetus through the placenta and umbilical vein • AFB recovered from decidua, amnion and chorionic villi
Congenital Tuberculosis • Criteria for Diagnosis: • Proven tuberculosis lesions in infant plus: • Lesions in the 1st week of life, or • Primary hepatic complex, or • Maternal genital tract or placental tuberculosis, or • Exclusion of postnatal transmission • Placenta: granulomatous deciduitis, intervillous abscesses with AFB • High neonatal mortality due to delayed diagnosis and treatment • Active pulmonary TB during pregnancy adverse fetomaternal outcome
Tuberculous Peritonitis and Gastrointestinal Tuberculosis • Peritonitis - spread from adjacent disease (fallopian tube, intestine, mesenteric lymph node) or miliary disease • Diagnosis: fluid-culture, PCR, ADA; bx • Gastroenteritis • Ileocecal area – most typical site of enteritis • presents as mass or acute abdomen • diagnosis: biopsy/surgical resection-culture
Surgical Pathology Unknown Case Conference 3/26/07 Case 3: Candida Pneumonia in Patient with Immune Compromise
Candida Pneumonia • Low prevalence • ICU 1992-97(N=4389): 7.8% all fungi (mainly Candida), bacteremic patients 1986-93 = 4% • Immunosuppression – neutropenic, DM, steroids, cirrhosis, HIV • Prior lung infection/disease • Mainly a colonizer and not the cause of disease
Candida pneumonia • Two main forms • Primary: local or diffuse BN from endobronchial inoculation of lung-rare • Secondary: hematogenous seeding with finely nodular diffuse lung infiltrate • Other forms • Necrotizing pneumonia mycetoma, transient infiltrates, URI, “empyema thoracis”
Candida Pneumonia • Diagnosis • X-ray and CT scan – nonspecific • Sputum, ET aspirate, BAL culture – indefinite • Biopsy demonstrating lung tissue invasion by fungi + positive culture* = definitive diagnosis *Culture: C. albicans = 40-70% 1° candida pneumonia
Candida Pneumonia • Histopathology • Primary • Evidence of aspiration • Evidence of Candida invasion into bronchial wall with or without destruction of resp.ep. • Secondary • Microabscesses with pseudohyphae penetrating vessels, and • Evidence of pseudohyphae invading lung interstitium and airways
Candida Pneumonia • Gross and microscopic pathology • Hematogenous: miliary nodules with central necrotizing inflammation and hemorrhagic rim • Aspiration: bronchopneumonia with fungi in airways or bronchocentric granulomatous inflammation • Candida glabrata in tissue: yeast only w/o pseudohyphae
Surgical PathologyUnknown Case Conference3/26/07 Case 4: Disseminated Aspergillosis s/p XRT for Clear Cell Sarcoma in AIDS Patient
Aspergillosis • Patterns of Pulmonary Aspergillosis • Colonization (fungus ball) • Hypersensitivity (ABA, eosinophilic pneumonia, bronchocentric granulomatosis, hypersensitivity pneumonitis) • Invasive (acute, necrotizing pseudomembranous tracheobronchitis, chronic necrotizing PNA, BP fistula, empyema)
Aspergillosis • Invasive disease = angiocentric hemorrhagic infarction with characteristic hyphae • Dichotomous branching at 45° • Septation • 3-6 um wide • +/- characteristic fruiting head • Differentiate from: *Fusarium spp, Zygomycete, Candida spp, P. boydii
Clear Cell Sarcoma • Rare sarcoma of young adults with melanocytic/uncertain differentiation • Initially in the extremities, often recurrent and/or metastatic • t(12;22)(q13;q12) = EWS/ATF1 fusion
Surgical Pathology Unknown Case Conference 3/26/07 Case 5 Intestinal Mycobacterial Infection
Intestinal Mycobacterial Infection • Endoscopy +/- biopsy = enteritis with unusual clinical features • Similar infectious agents affect the small bowel and colon with some exceptions • Attempt specific diagnosis of infectious agent using special stains or molecular techniques
Enteric Mycobacterial Infection • M. tuberculosis • Re-emerging • Primary GI or miliary with lung disease • Ileocecal/jejunoileal/appendix/asc.colon • Nontuberculous mycobacteria (MAI) • HIV/AIDS • Disseminated with GI involvement • Small bowel/colon/mesenteric nodes
Enteric Mycobacterial Infection • M. tuberculosis • Multiple ulcers/strictures with skip areas • Caseating (transmural) granulomas with hyalinization/calcification and aphthous ulcers with rare or no AFB • MAI • HIV: diffuse histiocyte infiltration, rarely granulomas (with or without necrosis) • Abundant AFB