Download
1 / 16
180 likes | 352 Views
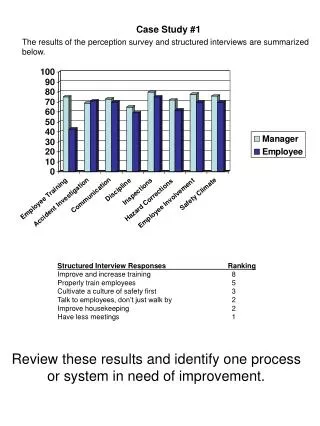
Case Study 1. 55-year-old man is referred for mild lymphadenopathy and lymphocytosis found during routine medical examination. Findings: Patient has 2-3 cm bilateral adenopathy in cervical and axillary chains Spleen and liver are not palpable

E N D
Case Study 1 55-year-old man is referred for mild lymphadenopathy and lymphocytosis found during routine medical examination • Findings: • Patient has 2-3 cm bilateral adenopathy in cervical and axillarychains • Spleen and liver are not palpable • Patient is asymptomatic except for occasional night sweats • Performance score is excellent • CBC count: • WBC count 36,000/µL (79% mature lymphocytes, ANC 2,800 cells/mm3) • Hgb 12.5 g/dL • Platelets 167,000/µL • Flow cytometry consistent with CLL CBC, complete blood cell; WBC, white blood cell; ANC, absolute neutrophil count; Hgb, hemoglobin.
Question 1 What treatment would you recommend for initial therapy? • Observation • Chlorambucil ± prednisone • Chlorambucil + obinutuzumab • Fludarabine + rituximab • Bendamustine + rituximab • Fludarabine, cyclophosphamide + rituximab • Pentostatin, cyclophosphamide + rituximab
Case Study 1 (cont.) • The patient is observed for the next 2 years then progressive fatigue and dyspnea on exertion develop • CBC: • WBC 96,000/µL (87% mature lymphocytes, ANC 4,500 cells/mm3) • Hgb 9.5 g/dL • Platelets 87,000/µL • Evaluation for hemolysis and ITP is negative • No evidence of GI blood loss • Cytotoxic therapy is started • Patient is now 60 years old CBC, complete blood cell; WBC, white blood cell; ANC, absolute neutrophil count; Hgb, hemoglobin; ITP, idiopathic thrombocytopenic purpura.
Question 2 Prior to starting therapy, which of the following prognostic tests would be most important to perform? • None; the patient progressed quickly so we know his prognosis is limited • β2-microglobulin • IgVH mutational status • ZAP-70 status • FISH analysis • CD38 expression IgVH, immunoglobulin heavy chain variable; ZAP-70, zeta-chain–associated protein kinase 70; FISH, fluorescence in situ hybridization.
Case Study 1 (cont.) • FISH analysis is performed and shows del(11q) in 57% and del(17p) in 6% of cells FISH, fluorescence in situ hybridization.
Question 3 What treatment would you recommend at this time? • Observation • Chlorambucil ± prednisone • Chlorambucil + obinutuzumab • Alemtuzumab ± rituximab • Fludarabine + rituximab • Bendamustine + rituximab • Fludarabine, cyclophosphamide, + rituximab • Pentostatin, cyclophosphamide ,+ rituximab
Case Study 1 (cont.) • The patient is treated with FCR and achieves a partial response • The patient does well for the next 18 months, but then progresses and symptomatic anemia requiring therapy develops again • The patient is now 62 years old • Prior to retreatment, FISH analysis was performed and shows del(11q) in 27% and del(17p) in 86% of cells • FCR, fludarabine, cyclophosphamide, + rituximab; FISH, fluorescence in situ hybridization.
Question 4 What treatment would you recommend for second line? • Observation • Chlorambucil + obinutuzumab • Alemtuzumab ± rituximab • Fludarabine + rituximab • Bendamustine + rituximab • Fludarabine, cyclophosphamide, + rituximab • Pentostatin, cyclophosphamide ,+ rituximab • Ibrutinib
Case Study 2 76-year-old woman with diabetes and chronic stable angina • Referred for mild lymphadenopathy and lymphocytosis found during annual medical exam • Findings: • 2 cm adenopathy in the cervical, axillary, and inguinal chains • Spleen is palpable 4 cm below left costal margin • Completely asymptomatic • Performance score is good • CBC count • WBC count 23,000/µL (81% mature lymphocytes, ANC 3,500 cells/mm3) • Hgb 13 g/dL • Platelets 181,000/µL • Flow cytometry is consistent with CLL • FISH analysis shows del 13qin 52% of cells, unmutated • β2-microglobulin of 3.4 µg/mL, negative for ZAP-70 CBC, complete blood cell; WBC, white blood cell; ANC, absolute neutrophil count; Hgb, hemoglobin; FISH, fluorescence in situ hybridization; ZAP-70, zeta-chain–associated protein kinase 70.
Question 1 What treatment would you recommend for initial therapy? • Observation • Chlorambucil ± prednisone • Chlorambucil + obinutuzumab • Fludarabine + rituximab • Bendamustine + rituximab • Fludarabine, cyclophosphamide, + rituximab • Pentostatin, cyclophosphamide, + rituximab
Case Study 2 (cont.) • Patient is observed for the next 6 years • Eventually progressive fatigue and dyspnea on exertion develops; she is now 82 years old • Patient had a mild stroke 2 years ago but has largely recovered • CBC count now shows: • WBC count 126,000/µL (91% mature lymphocytes, ANC 6,300 cells/mm3) • Hgb 8.9 g/dL • Platelets 107,000/µL • Evaluation for hemolysis is negative • There is no evidence of GI blood loss • FISH analysis repeated prior to starting therapy, showed del(13q) in 68% of cells • Together with the patient, it has been decided it is time to start cytotoxic therapy CBC, complete blood cell; WBC, white blood cell; ANC, absolute neutrophil count; Hgb, hemoglobin; FISH, fluorescence in situ hybridization.
Question 2 What treatment would you recommend at this time? • Observation • Chlorambucil ± prednisone • Chlorambucil + obinutuzumab • Fludarabine + rituximab • Bendamustine + rituximab • Fludarabine, cyclophosphamide, + rituximab • Pentostatin, cyclophosphamide,+ rituximab
Case Study 2 (cont.) • Patient is treated with chlorambucil and obinutuzumab and achieves a high-quality partial response • She does well for the next 3 years but symptomatic anemia that does not respond to treatment ultimately develops • Patient is now 84 years old with an ECOG PS of 2 ECOG = Eastern Cooperative Oncology Group.
Question 3 Prior to retreatment, which of the following prognostic tests would be most important to perform? • None; at relapse in an older patient, these tests have little practical utility • β2-microglobulin • IgVH mutational status • ZAP-70 status • FISH analysis • CD38 expression IgVH, immunoglobulin heavy chain variable; ZAP-70, zeta-chain–associated protein kinase 70; FISH, fluorescence in situ hybridization.
Question 4 What treatment would you recommend for second line? • Observation • Chlorambucil + obinutuzumab • Alemtuzumab ± rituximab • Fludarabine + rituximab • Bendamustine + rituximab • Fludarabine, cyclophosphamide, + rituximab • Pentostatin, cyclophosphamide, + rituximab • Idelalisib + rituximab • Ibrutinib
Case Study 2 (cont.) • The patient is treated with ibrutinib • She shows improvement in anemia and lymphadenopathy, and otherwise has stable disease