Download
1 / 19
450 likes | 1.47k Views
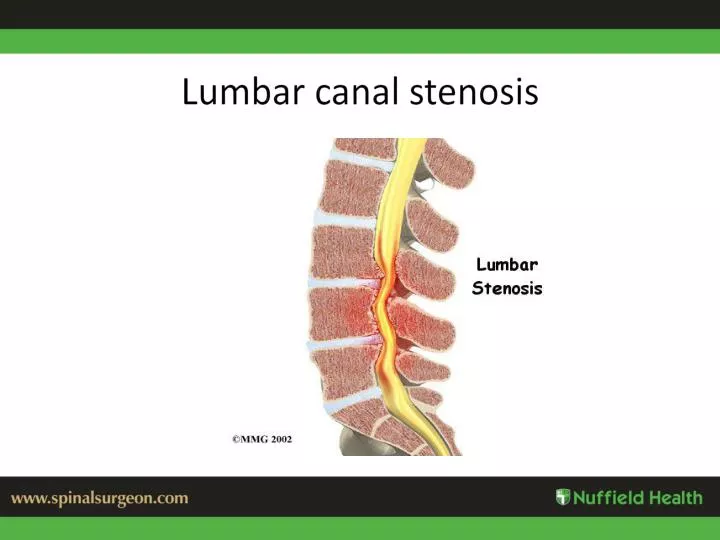
Lumbar canal stenosis. Causes of Stenosis. Degenerative spondylo-listhesis Facet subluxation and hypertrophy Pagets disease Tumour Facet joint cyst Congenital- achondroplasia Scoliosis with lateral shift. Differential Diagnosis. Vascular Claudication Hip OA

E N D
Causes of Stenosis • Degenerative spondylo-listhesis • Facet subluxation and hypertrophy • Pagets disease • Tumour • Facet joint cyst • Congenital- achondroplasia • Scoliosis with lateral shift
Differential Diagnosis • Vascular Claudication • Hip OA • Lumbar disc protrusion • MS • Tumour • AV malformation • Peripheral Neuropathy
Types of Stenosis • Central: No pain, but legs ‘slow’ on walking • Lateral recess: Unilateral leg pain, increased on walking.
Diagnosis Congenital Stenosis Traumatic Stenosis Infectious Stenosis
Diagnosis Degenerative Stenosis
JT. Right L45 Facet Joint Cyst. Severe Right sided leg pain and Low back pain Treated with decompression surgery
65/M. Pagets Disease causing stenosis. Long standing LBP. Neurogenic claudication distance 50 yards
Symptoms • 70% also have back pain • Leg pain worse on walking and standing and eased on sitting or bending forwards • Can cycle or walk leaning forwards on a trolley • Gradually Progressive • Increased on walking on hard surfaces , down an incline and in high heels
Tandem Stenosis • In 15-20% of patients both cervical and lumbar stenosis are present • Hoffman Sign positive. • Heel-Toe gait – poor balance. • Usually operate on the neck first
Signs • Minimal!! • One of the hallmarks of these patients is that they have no spinal tenderness, a full range of movement, SLR is normal and there is no neuro-deficit. • Diagnosis is purely in the history
Spinal Stenosis- what’s new? • Diagnosis often missed as no positive examination findings • Diagnosis on history: difficulty walking with cramps in legs, eased on sitting • Epidural injections- short term relief • Surgery- Now never do a laminectomy alone- alters the biomechanics • Always add dynamic stabilization- excellent outcomes
When to refer? • Pain uncontrolled in primary care • Walking getting progressively worse • Surgery is straight forward • No increase in surgical risk due to age.
Treatment • Conservative -Rest, analgesics, anti-inflammatories, oral steroids, antispasmodics, physiotherapy, weight loss, steroid injections
Treatment- Laminectomy and Dynamic Stabilization( my preferred option)
Complications and Outcomes of Surgery • 2-4% risk of infection, CSF leak , and Neural Injury • No death, or paralysis in 17 years of practise in over 4000 cases • Surgery has become safer, outcomes better and recovery quicker • 80% better on average • Increased age alone does not result in increased risk of surgery
Dynamic Stabilization • 29 elderly patients with degenerative scoliosis. Decompressivelaminectomy and dynamic stabilization without fusion. (Dynesis) • 54 month mean follow up. Oswestry score improvement of 51.6%. 51.7% improvement in VAS leg pain, and 57.8% for VAS back pain. Sivestre M, Lolli F, Bakaloudis G. Dynamic stabilization for degenerative lumbar scoliosis in elderly patients. Spine 2010 Jan
Dynamic Stabilization • 100 patients. Decompression and pedicle screw based dynamic stabilization (Cosmic) • Improved disability scores. ODI pre-op of 51, and post-op of 21. • Improvement in pain. VAS pre-op 6.5 and post-op 2.1. • SF-36 outcomes were also improved. Stoffel M, Behr M, Reinke A, Meyer B. Pedicle screw-based dynamic stabilization of the thoracolumbar spine with the Cosmic-system: a prospective observation. AchtaNeurochirurg 2010 May