Download
1 / 21
220 likes | 480 Views
Common Clinical Problems: Edema. A patient presents with BLE edema… what is she most likely to have?. Cause #1: Increased systemic hydrostatic pressure. Congestive heart failure Systolic or diastolic LV dysfunction RV failure, due to LV failure or pulmonary disease Constrictive pericarditis

E N D
A patient presents with BLE edema… what is she most likely to have?
Cause #1:Increased systemic hydrostatic pressure • Congestive heart failure • Systolic or diastolic LV dysfunction • RV failure, due to LV failure or pulmonary disease • Constrictive pericarditis • Restrictive cardiomyopathy • Valvular heart disease
Cause #2: Increased local hydrostatic pressure • Chronic venous insufficiency • Deep vein thrombosis • Portal hypertension/cirrhosis • Compression of IVC or iliac vessels • Mass • Pregnancy
Cause #3: Sodium and water retention by the kidney • Heart failure ( effective circulating volume) • Renal failure (including most cases of nephrotic syndrome in adults) • Cirrhosis • Pregnancy
Cause #4: Decreased plasma oncotic pressure • Cirrhosis • Malnutrition • Malabsorption • Nephrotic syndrome • Preeclampsia
Cause #5: Lymphatic obstruction • Malignancy • Filariasis • Post-surgery (especially mastectomy) or radiation • Typically unilateral
Cause #6: Increased capillary permeability • Usually clinically obvious • Infection • Anaphylaxis • Burns
Other causes • Drugs • Thyroid disease • Lipedema
Notes: • Some diseases can cause edema via more than one mechanism • Patients may have more than one contributing disease
Causes of Leg Edemafrom “The Patient History: Evidence Based Approach”, ed. Tierney & Henderson, Lange 2005 • Venous stasis/varicose veins 30% • Congestive heart failure (R or L) 30% • Lipedema 10% • Cirrhosis 10% • Nephrotic syndrome 5% • DVT or venous obstruction 3% • Medications 3% • Lymphatic obstruction 1% • Malnutrition/protein losing enteropathy 1%
Venous stasis • Etiology • Varicose veins • Incompetent venous valves • Postphlebitic syndrome (DVT) • Edema • Hemosiderin deposition • May develop • Stasis dermatitis with erythema and pain • Chronic ulcers Image from: http://www.sierravein.com/vein-disorders/venous-stasis-ulcers.htm
Lipedema • Fat deposition rather than true edema • Typically stops at the malleoli • The feet usually appear normal
Medications that cause edema • Calcium channel blockers • Amlodipine, felodipine, nifedipine • Direct vasodilators • Minoxidil, hydralazine, diazoxide • Glitazones • NSAIDs • Hormones • Corticosteroids, progesterone, testosterone
JVP is a key exam finding Is JVP elevated? • The edema is due, at least in part, to • primary cardiac disease OR • lung disease with R heart failure OR • Renal failure with sodium retention (which will be obvious when you check labs) Is JVP normal? • The edema is most likely due to • Venous stasis • Cirrhosis • Lipedema • Medications
Congestive Heart Failure Suggestive History • Dyspnea • Orthopnea • Paroxysmal nocturnal dyspnea • Edema • History of hypertension (diastolic dysfunction) • History of MI (systolic dysfunction) • Severe lung disease (RV failure)
Congestive Heart Failure: Exam + LR - LR • PMI lateral to MCL 5.8 NS • S3 5.7 NS • HR > 100 5.5 NS • Elevated JVP 3.9 NS May be present but not diagnostically helpful: • Edema NS NS • Crackles NS NS • S4 NS NS McGee, Evidence Based Physical Dx
Other exam that would suggest cirrhosis • Jaundice • Ascites • Splenomegaly • Gynecomastia (failure to clear estrogen) • BUT remember that cardiac disease can cause hepatic congestion and cirrhosis. IN THIS CASE JVP SHOULD BE ELEVATED
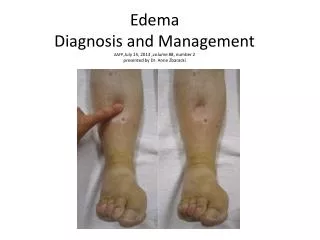
What if the edema is unilateral? • DVT should be excluded • Venous stasis • Injury to or compression of venous or lymphatic system of that leg • Patients with diseases that cause bilateral edema may develop it first in one leg, usually the left
What if the edema is periorbital? • Suggests nephrotic syndrome with severe hypoalbuminemia http://www.ask.com/wiki/Dropsy