Download
1 / 15
150 likes | 271 Views
Depression. Pathology / Pharmacology Quiz. Question 1. Explain the monoamine theory of depression. Answer 1.

E N D
Depression Pathology / Pharmacology Quiz
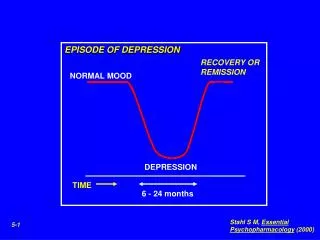
Question 1 • Explain the monoamine theory of depression
Answer 1 • Monoamine Theory of Depression – that depression is caused by a functional deficit of monoamine transmitters at certain sites in the brain (and that mania is caused by a functional excess). • 5-HT (serotonin) is the key mediator, but NA is also involved, and pharmacological evidence supports this, however there are several anomalies. Clinically, it appears that inhibitors of 5-HT uptake and inhibitors of NA uptake are equally effective as antidepressants, although individual patients may respond better to one or the other. DA may be peripherally involved as well. • Several drugs are not effective when they otherwise might be thought to be. E.g. supplying a NT precursor will not increase NT levels unless the precursor levels are the rate-limiting step. Similarly, if the nerve terminals are functionally defective, increasing NT in the terminal will not increase NT in the synapse. • Also, the anti-depressant effect of these drugs takes weeks to develop, suggesting that the secondary, adaptive changes in the brain (rather than the primary drug effect) are responsible for the clinical improvement. Therefore monoamines should not be viewed as ‘happy’ or ‘sad’ chemicals in the brain, but as regulators of long-term trophic effects, the time of such effects is paralleled by mood changes. • Major evidence for the monoamine theory of depression is: • Drugs which deplete monoamine stores such as reserpine can cause depression • 5-HT receptor densities are increased in the brain tissue of suicide deaths, and this is thought to be linked to low endogenous levels of serotonin • Depressed patients show lower than normal concentrations of serotonin metabolites in their CSF • In depressed patients, NA transmission is reduced in both of the principle noradrenergic centres – the locus coeruleusand the caudal raphe nuclei • 5-HT transmission is reduced in the caudal raphe nuclei and the rostral raphe nuclei.
Note: NA is removed from the synapse either by (A) presynaptic reuptake by Uptake 1 (NET – norepinephrine transporter) and metabolism by MAO (monoamine oxidase – bound to surface of mitochondria), or (B) metabolism by COMT (catechol-O-methyl transferase) both extracellularly and intracellularly, or (C) via the postsynaptic Uptake 2, however the specificity for NA is low and Uptake 2 is not prominent in the CNS
Question 2 • Tricyclic antidepressants (such as imipramine) inhibit: • SERT only • NET only • SERT and NET • SERT, NET, mAChR but not alpha1R • SERT, NET, mACHr, alpha 1R but not H1 • SERT, NET, mAChR, alpha 1R and H1
Question 3 • Describe the effects of antagonists acting on: • mAChR • H1R • D2R • Alpha1 R • mAChR
Question 4: • Which of the following is a common side effect of SSRIs (such as fluoxetine) monotherapy? • Hyperthermia • Loss of libido / orgasm • Hypertension • Tremor • Muscle rigidity
Question 5 • Compared to fluoxetine, venlafaxine’s adverse effect profile has an increased risk of: • Tremor • Suicide • Impotence • Urinary retention • Tardive dyskinesia
Question 6 • MAO-A has substrate preference for ____ whereas MAO-B has substrate preference for _____ • Phenelzine covalently binds to _____ and irreversibly inhibits it, whereas selegiline competitively inhibits ____ • Note: Selegiline has recently been approved as a transdermal patch and is safer than phenelzine • Hint: Selegiline is the drug of choice for comorbid Parkinson’s and depression
Question 6 • MAO-A has substrate preference for 5-HT whereas MAO-B has substrate preference for DA • Phenelzine covalently binds to both MAO-A and MAO-B and irreversibly inhibits them, whereas selegiline irreversibly inhibits MAO-B • Note: Selegiline has recently been approved as a transdermal patch and is safer than phenelzine
Question 7 • Explain the mechanism of action of mirtazipine
Question 7 - Answer • Mirtazipine is a noradrenergic and specific serotonin antidepressant (NaSSAs) • These have a dual mechanism of action – they increase levels of 5HT and NA in the synapse to normal ranges. They inhibit both α2Adr autoreceptors and heteroreceptors, thus preventing negative feedback of NA on 5-HT and NA, increasing neurotransmission. • They also block 5HT2 and 5HT3 receptors on the post-synaptic membrane, causing enhanced5HT1 mediated neurotransmission. • AE include drowsiness, dry mouth, increased appetite and weight gain. Their inhibition is not irreversible, but they do slow the clearance of NA and 5HT from the synaptic cleft.