Download
1 / 27
440 likes | 1.03k Views
Campylobacter. Spirally small, curved, G- ve , Motile, NS, NC bacteria. They are comma, S, or “gull-wing” shaped spiral rods. Motile by single polar unsheathed flagellum at one or both ends.

E N D
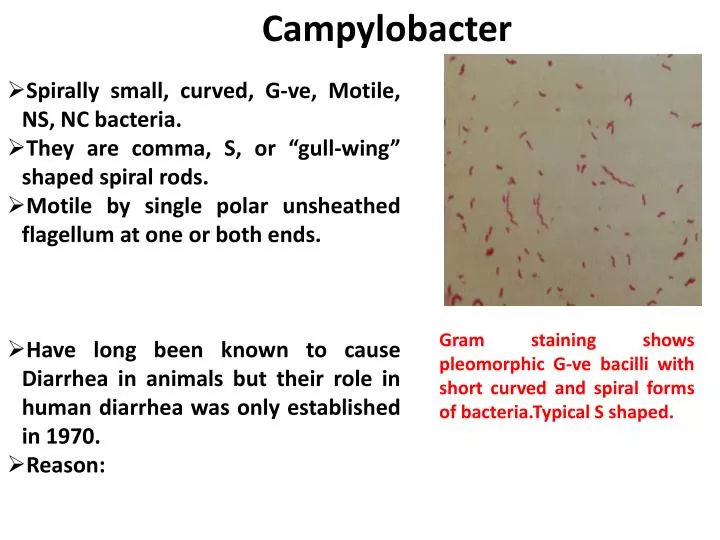
Campylobacter • Spirally small, curved, G-ve, Motile, NS, NC bacteria. • They are comma, S, or “gull-wing” shaped spiral rods. • Motile by single polar unsheathed flagellum at one or both ends. • Have long been known to cause Diarrhea in animals but their role in human diarrhea was only established in 1970. • Reason: Gram staining shows pleomorphic G-ve bacilli with short curved and spiral forms of bacteria.Typical S shaped.
Coloured scanning electron micrograph (SEM) of a Campylobacter jejuni bacterium. This motile, Gram-negative bacterium possesses long flagella, at either end, which enable it to move
Campylobacter is the second most common cause of bacterial foodborne illness in the United States after Salmonella
16 Species Medically important are C.jejuni, C.coli, C.upsaliensis: Causing human diarrhea. C.fetus : Cause extraintestinal infection. C.sputorum, C.rectus: Periodontal disease.
Culture Characteristics Campylobacter are microaerophilic thermophilic*(growing well at 420C) Capnophilic(require 10% CO2 ) Survive in Cary Blair media. Selective Media: 1. Modified Skirrow Media contining blood agar base, & antibiotics (Vancomycin, Trimethoprim, and Polymyxin B). 2. Campy-Brucella agar with antibiotics Rectal swab or stool swab or 1 or 2 drop of liquid stool specimen are inoculated directly on the surface of the agar medium. Incubation: 420 C for 48 to 72 hours.
Culture characteristics Colonies are flat grey, irregular shaped and moist/ glistening entire edges.
Epidemiology Campylobacter infection: Zoonotic with variety of animal serving as reservoir Chickens, domestic animals (Cattle and Swine) and birds. Source of infection is food of animal origin, especially raw milk. It is part of the normal intestinal flora of domestic animals and birds and is shed in their feces. Contaminated poultry are responsible for more than half of the Campylobacter infection. Human acquire infection with C.jejuni and C.coli after consumption of contaminated food, milk or water. Once a person is infected, the organism can be transmitted from person to person by faecal-oral route. Incidence rate high among children less than 2 year old and young adults(20 to 40 years old).
Pathogenesis & Immunity • Infectious dose and host immunity determine whether gastroenteric disease develops • Some people infected with as few as 500 organisms while others need >106 CFU • Pathogenesis not fully characterized • No good animal model • Damage (ulcerated, edematous and bloody) to the mucosal surfaces of the jejunum, ileum, colon • Inflammatory process consistent with invasion of the organisms into the intestinal tissue; M-cell (Peyer’s patches) uptake and presentation of antigen to underlying lymphatic system • Non-motile & adhesin-lacking strains are avirulent
Pathogenicity • Occurs with in 2-4 days(range of incubation period, 1-7 days) of ingestion of contaminated food, milk or water. • Cause acute gastroenteritis, last for days to several weeks, usually self limiting. • Infection first jejunum and ileum and later spread distally to affect terminal ileum, colon and rectum • C.jejuni is invasive, multiply in small intestine, penetrate gut epithelium and disrupt fluid absorption. • Virulence factor: Produce enterotoxin • cytotoxin • Adhesions • Intracellular survival • Ability to penetrate cells
Clinical feature Fever, headache, myalgia and intestinal– abdominal cramping and watery diarrhoea with or without blood. Cause both traveller’sdiarrhoea and pseudo appendicitis. Complication include GuillainBarre syndrome(GBS), septic abortion and reactive arthritis. GBS associated with specific C.jejuni serotype O:19.
GBS(Guillain-Barre Syndrome) • C.jejuni most recognized antecedent cause of GBS, an acute paralytic disease of the peripheral nervous system. • 20-40% of GBS patients are infected with C.jejuni which may appear 1-2 weeks after the onset of acute campylobacter illness. • It is believed that antigenic cross reactivity between surface lipopolysaccharides of some strains of campylobacter and peripheral nerve gangliosides. Thus antibodies directed against specific strains of Campylobacter can damage neural tissue in peripheral nervous system.
Laboratory Identification • Specimen Collection and Processing: • Feces refrigerated & examined within few hours • Rectal swabs in semisolid transport medium • Blood drawn for C. fetus • Microscopy: • Gull-wing appearance in Gram stain • Darting motility in fresh stool • Fecal leukocytes are commonly present • Culture • Feces/ rectal swab plated on selective media(Butzler’s selective medium, Skirrow Campylobacter selective medium, Campy BAP. • Growth at 37o, or 42-43oC. • Colonies typically flat, effuse & tendency to spread on moist agar. Nonhaemolytic, grey or colorless, moist and flat.
Identification: • Growth at 25o, 37o, or 42-43oC • Hippurate hydrolysis (C. jejuni is positive). • 1% Sodium Hippurate+ Suspected isolate colonies • Indicator Ninhydrin is added to detect glycine by turning inoculated broth deep purple colour. 370C Benzoic acid +Glycine 2hours
Serology & Molecular test CFT & ELISA: Detect recent infection with C.jejuni or C.coli. PCR amplification of the 16S rRNA gene and sequencing . Treatment Gastroenteritis, Infection is self-limited and is managed by fluid and electrolyte replacement. Severe gastroenteritis treated with erythromycin and Ciprofloxacin. Prevention Potentially contaminated food, such as poultry, should be throughly cooked, and milk and milk prodcuts should be pasteurised.
Helicobacter • First observed in 1983 as Campylobacter-like organisms (formerly Campylobacter pyloridis) in the human stomachs of patients peptic ulcer disease(PUD) and gastric cancer. • Helicobacter pylori is the prototype organism in this group. It is associated with antral gastritis, duodenal ulcer disease, peptic (gastric )ulcers, and gastric carcinoma.
H.pylori Gram negative spirally curved bacilli, NS. Spheroid or coccoid in old culture. Very Motile corkscrew motion with a unipolar tuft of lophotrichous flagella(Other Helicobacter posses multiple bipolar sheathed flagella). Culture: Microaerophilic, 5-10% CO2 & high humidity. Growth at 370C, not 250C or 420C. Can grow in Skirrow Campylobacter selective medium. Produces circular, convex and translucent colonies after 3-7 days. Biochemical : Urease production(Rapid diagnostic). Catalase, Oxidase production Does not metabolize carbohydrates or reduce nitrates.
Colonises the gastric mucosa of almost 50% of the adult population. Adapted to human gastric mucosa. • Though contraversial but claims, human acquired infection as zoonoses from the stomach of other mammals (cat, dog, mice rats etc) each with its own helicobacter species. • Person to person transmission by oral-oral and faecal-oral routes. • Important Human Pathogens: • Helicobacter pylori , H. cinaedi, H. fenneliae
Virulence factors • H.pylori produce cytotoxin which cause vacuolation of gastric mucosa. • Cag , pathogenicity gene island, a group of genes consist of cag encoding for cag A protein, and vac(vacuolatingcytotoxin gene) along with over 40 genes. • Cag A is injected by H.pylori into human gastric epithelial cell and affect the host cell protein expression inducing cytokine release, cytoskeletal changes and proliferation to enable H.pylori to successfully colonise gastric epithelium. • Urease released by H.pylori producing ammonia ions that neutralise stomach acid in the vicinity of the organism, thus favoring bacterial multiplication. • Bacterial antigen cross react with antran gastric antigen stimulating an autoimmune response. • Protease produced by the organism degrade gastric mucosa.
Pathogenesis H.Pylori colonizes surface of gastric mucosa, especially antrum(Any part may be colonized).Bacteria present in large numbers in mucus overlying mucosa(pH=7.0). Exact pathogenic mechanism not known. Bacterial protease, toxins or ammonia or autoimmune responses may all contribute. Where numerous, underlying mucosa shows a superficial gastritis known as type B gastritis.
H.Pylori is associated with antral gastritis, duodenal(peptic) ulcer disease, gastric ulcers. Can also cause gastric malignancies, namely ‘Adenocarcinoma’ and gastric B cell lymphoma( mucosa associated lymphoid tissue(MALT) lymphomas).
Laboratory diagnosis Endoscopy and biopsy
Rapid urease test: A biopsy sample is placed into a urea broth and an indicator such as phenol red. The urease produced by H. pylori hydrolyzes urea to ammonia, which raises the pH of the medium, and changes the color of the specimen from yellow (NEGATIVE) to red (POSITIVE). Microscopy: Gram / Giemsa / Warthin-Starry silver stain H.Pylori in gastric mucosal impression smear(SilverStaining)
Culture: • Histology more sensitive than culture. • Usually not done. • Only done when sensitivity tests or typing is required. • Tissue biopsy material is collected in Stuart transport media and cultured in selective media. • Antigen detection • Faecal antigen detection by ELISA(Commercial-Meridian Diagnostic, USA). • PCR. • Urea breath test - samples of breath air are collected by having the patient blow into a tube before and 30 min after ingestion of 13C-labeled urea, rapid, noninvasive, for assessing response 4-8w post therapy, expensive but non invasive!!
Treatment • PPI proton pump inhibitors therapy omeprazole / lansoprazole +amoxicillin + clarithromycin or metronidazole + Bismuth subsalicylate
Reference: www.Slideshare.com