Download
1 / 44
440 likes | 858 Views
Shunt malfunction. Classification of shunt malfunction. Mechanism Mechanical vs Functional Time of occurrence Early vs Late Site of malfunction Causes of malfunction Surgeon, Patient, Shunt. 1.0. .9. P = posterior (60 cases). .8. A = anterior (61 cases). .7. .6. .5. .4. 0.

E N D
Classification of shunt malfunction • Mechanism • Mechanical vs Functional • Time of occurrence • Early vs Late • Site of malfunction • Causes of malfunction • Surgeon, Patient, Shunt
1.0 .9 P = posterior (60 cases) .8 A = anterior (61 cases) .7 .6 .5 .4 0 1 2 3 4 5 6 • Shunt Survival Function Chicago prospective study C u m S u Oregon H S U (275 cases) Toronto-Paris (1552 cases) Denmark (884 cases) r P v i v A a l DURATION
F 2800 o l 2400 l o 2000 w - 1600 u p 1200 800 400 0 N = 334 88 42 28 68 15 21 "Overdrainage" Migration Obstruction XX Underdrainage Fracture Improper placement B & W plots - Follow-up/Event DP Shunts (Toronto-Paris) - First insertion
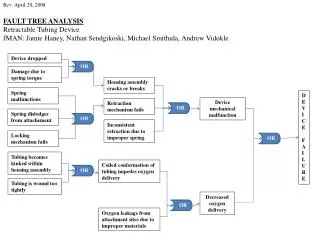
Causes of shunt complications • Early shunt complications • Surgical technique • Improper placement • Disconnection • Migration • Skin problems • Debris in the CSF • Early Obstructions • Shunt • Acute overdrainage
Causes of shunt complications • Late shunt complications • Chronic overdrainage • Hydrodynamic characteristics • Mechanical stress on the device • Connectors • Deterioration of the distal tubing Proximal obstruction Migration & fracture
Delayed Proximal obstruction is correlated with chronic overdrainage Slit Normal Enlarged None 55.7 78.3 63.9 S. Failure 44.3 21.7 36.1 Ventr. Obstr. 81.3 8.1 21.4
Consequences of overdrainage • Rare : « slit ventricle syndrome » Epstein 1980 • Very common : proximal obstruction
« Slit ventricle syndrome » • Recurrent episodes of ICH despite a patent shunt • Rare > 0.5% (10/3000) • Loss of volumetric buffering reserve • Treatment • Increase the valve resistance • Cranial expansion
Proximal obstruction • Very frequent • ICH with small ventricles at the beginning (Laplace’s law) • Shunt revision
= = Equivalence
Hypothetically….Prevention of late shunt malfunction by : Prevention of deterioration of the distal tubing Prevention of chronic overdrainage
Prevention of deterioration of the distal tubing • Integral distal tubing - no connectors • Striped distal tubing
Past Present The silent revolution
Hypothetically….Prevention of early shunt malfunction by : ?
Answer :Series of 946 new cases of hydrocephalus in childhood (1987-2002) 15 years of hydrocephalus treatment at Necker Thanks to Ricardo and Mercia
Series characteristics • Age • Median 184 day • Etiologies
Third V. - results • Success 66.5% • Factors correlated with success (Cox) • Variable in the equation : ETIOLOGY • Tumors 84% • Meningitis 20% • Not in the equation : SURGEON, PATIENT’S AGE
Survival Function - Third ventriculostomy 1.0 .9 .8 .7 .6 Cum Survival .5 .4 .3 .2 .1 0.0 0 720 1440 2160 2880 3600 360 1080 1800 2520 3240 Follow-up
First shunt characteristics- all OSV - • Type • VP / VA 667 / 1 • Right / Left 579 / 88 1 bilateral • Tip location • Correct 580 • Questionable 88
Shunts - results • No complications 411 61.5% • Infection 49 7.3% • Mechanical complic. 208 31.1%
Survival Function - valve OSV Probability of survival 45.9% at 15 years 1.0 .9 .8 50% at 12 yrs = 2.5 M$ saved .7 .6 .5 .4 .3 .2 Cum Survival .1 0.0 0 720 1440 2160 2880 3600 4320 5040 360 1080 1800 2520 3240 3960 4680 5400 Follow-up
1.0 .9 .8 .7 .6 .5 .4 .3 .2 .1 0.0 0 720 1440 2160 2880 3600 4320 360 1080 1800 2520 3240 3960 Survival Function - OSV vs. « DP shunts » Log Rank 0.000 OSV DP shunts Cum Survival Follow-up Dramatic decrease of late shunt complications,but number of early complications unchanged !
1.0 .8 .6 .4 .2 Cum Survival 0.0 0 720 1440 2160 2880 3600 4320 5040 360 1080 1800 2520 3240 3960 4680 5400 Follow-up Survival Functions - Ventricular tip location (correct vs questionable) « correct » « questionable »
Conclusions • Third ventriculostomy in 30% of the cases • Prevention of late shunt complications have been achieved by • limiting chronic overdrainage • using integral, “striped” distal tubing • Prevention of early shunt complications is largely up to us • Good surgical technique • Clean CSF • Appropriate hydrodynamic characteristics of the valve