Download
1 / 23
230 likes | 510 Views
Herpesviridae. By the Griswolds : Aite " Aunt Edna” Lander Abraham “Clark” Jeon Caitlin “Ellen” D’Souza Chris “Rusty” Moriarty Mathieu “ Audry ” Sabbagh. Herpesviridae … The Basics. Enveloped ds DNA virus Site of replication = nucleus 3 families

E N D
Herpesviridae By the Griswolds: Aite "Aunt Edna” Lander Abraham “Clark” Jeon Caitlin “Ellen” D’Souza Chris “Rusty” Moriarty Mathieu “Audry” Sabbagh
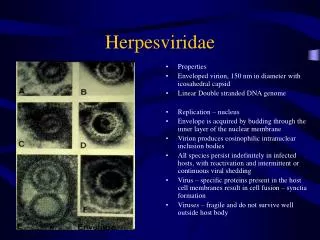
Herpesviridae… The Basics • Enveloped ds DNA virus • Site of replication = nucleus • 3 families • Alphaherpesvirinae (herpes simplex) • HSV1, HSV2, and VZV • Betaherpesvirinae • CMV, HHV6 • Gammaherpesvirinae (lymphoproliferative) • Epstein Barr virus
The Basics… Continued • Important characteristics • latent infections • HSV = neuronal tissue • CMV = non-neuronal tissue • Lymphproliferative =mucosal tissue • Some are associated with malignancies (i.e. Epstein-Barr virus can induce Burkitt’s lymphoma)
HSV-1 Epidemiology Most frequent in early childhood 70% infected by adulthood Transmission Oral infx (saliva) and genital infx (less common than HSV-2) Clinical presentation 1° infection: cleared by CTL’s (on MHC Class I) Sx Child = gingivostomatitis, fever, malaise Active infx cleared by CTL’s Lasts about 3 wks Adult = severe pharyngitis Lasts about 1 wk Note: Ig is NOT successful in eliminating infx
HSV-1 • Latency • along trigeminal nerve • transient active infx within DRG • 2° (recurrent) infx • prodrome of pain and tingling • Cold sore = cluster of blisters • Recurrences assoc with: • stress, UV light, ifx, menstruation, dec immunity • Less common: • Immune comp: Genital herpes, Encephalitis , Keratitis; Immune supp: pneumonia, severe mucocutaneous lesions • Dx: made clinically “grouped vesicles on an erythematous base” • Prevention = difficult (asymptomatic shedding, easily spread among toddlers) • Tx = Acyclovir
HSV-2 • Epidemiology • 25-35% in US infected • most cases are asymptomatic • Transmission • Genital infections • Oral infections (much less common than HSV-1) • Clinical presentation • 1° infx • Most cases = asymptomatic • Sx may include: • Painful vesiculoulcerative lesions • fever, malaise, and myalgia (more severe than with 1° oral ifx)
HSV-2 • Latency = same as HSV-1 • 2° (recurrent) infx = same as HSV-1 except: • Reactivation is more frequent • Shedding more likely asymptomatic • Dx: of HSV-2 = same as HSV-1 • Prevention • Abstinence • Monogamy • Condoms • Tx = Acyclovir
Neonatal Herpes • Most commonly caused by HSV-2 • Transmission • Transcervical • Most common = asymptomatic recurrent infx • Most dangerous = 1° infx (50% rate of transmission) • Transplacental = intrauterine distress • Manifestations • Skin, eye and mouth involvement = best outcome • Encephalitis, Disseminated disease, Neurologic or ocular sequelae • Dx: Maternal anti-HSV IgG, presence of any sx, viral isolation • Tx = IV acyclovir • Prevention • No routine screening is recommended • All pregnant women should be carefully examined at start of labor • For women with sx: C-section recommended
VZV • Varicella = chicken pox, Zoster = shingles • Epidemiology • Common infx = 97% adults are seropositive • Highly contagious • Incidence of zoster increases with age • Transmission = via respiratory droplets • Pathogenesis • initial infx of respiratory mucous • spread to regional lymph node • disseminate to liver and spleen • infect circulating monocytes • Within 14-21 days, infects capillary endothelial and skin epithelial cells
VZV • 1° infx = chickenpox • Prodrome of fever, malaise, HA, and abdominal pain • Classic presentation = 3 stages • New lesions = erythematousmaculopapules • Maturing lesions = vesicles/pustules • Healing lesions = scabs • Latency = same mechanism as with HSV-1 and HSV-2 • 2° (recurrent) infx = Zoster (shingles) • Painful vesicular rash within dermatome of a single spinal nerve • Post-herpetic neuralgia (RF = inc age and/or dec immunity)
VZV • Dx: clinical presentation • Tx: Chicken pox = symptomatic, Zoster = Acyclovir • Post-Herpetic Neuralgia = low dose TCA’s or anticonvulsants • Prevention : Live, attenuated vaccine for:Children<12 months and Seronegative adults; also, elderly
Board Review Stuff • Herpesvirus: enveloped double stranded linear DNA virus • HSV-1: Gingivostomatitis, keratoconjunctivitis, temperal lobe encephalitis (most common cause of sporadic encephalitis in the USA), herpes labialis • Transmitted respiratory secretions and saliva • HSV-2: Herpes genitalis, neonatal encephalitis • Transmitted sexual contact, perinatal • VZV (HHV-3): Varicella-Zoster (shingles along dermatomes), encephalitis, pneumonia • Transmitted by respiratory secretions
Board Review Stuff • Get herpes in a CHEVrolet • CMV • HSV • EBV • VZV • VZV remains dormant in the trigeminal and dorsal root ganglia • Treat HSV, VZV, EBV with Acyclovir • Acyclovir is monophosphorylated by HSV/VZV thymidine kinase and inhibits viral DNA polymerase • HSV/VZV mechanism of resistance against Acyclovir is a lack thymidine kinase
Questions • What is the mechanism of resistance by HSV and VZV against acyclovir? • Modified envelop protein • Mutated DNA polymerase • Mutated M2 protein • Lack thymidine kinase • Lack of viral kinase
Questions • What is the mechanism of resistance by HSV and VZV against acyclovir? • Modified envelop protein • Mutated DNA polymerase • Mutated M2 protein • Lack thymidine kinase • Lack of viral kinase
Question • 26 yo male presents with watery blisters in the mucus membrane of the mouth. Serum serology was performed and Dx of HSV-1 was made. HSV-1 is ? • A single stranded RNA virus • A double stranded RNA virus • As single stranded DNA virus • A linear single stranded RNA virus • A linear double stranded DNA virus
Question • 26 yo male presents with watery blisters in the mucus membrane of the mouth. Serum serology was performed and Dx of HSV-1 was made. HSV-1 is ? • A single stranded RNA virus • A double stranded RNA virus • As single stranded DNA virus • A linear single stranded RNA virus • A linear double stranded DNA virus
Question After a bout of the flu, a 35 year-old man notices several 0.3-cm, clear vesicles on his upper lip. The vesicles rupture, leaving shallow, painful ulcers that heal over the course of 4 weeks. Several months later, after a skiing trip, similar vesicles develop, with the same pattern of healing. Which of the following is most likely associated with these lesions? a. Biopsy specimen showing squamous epithelial hyperketatosis b. Positive serologic tests for Herpes Simplex 1 c. Peripheral blood smear showing atypical lymphocytes d. Biopsy specimen showing mononuclear inflammatory infiltrate e. Positive serologic tests for Varicella-Zoster virus
Question After a bout of the flu, a 35 year-old man notices several 0.3-cm, clear vesicles on his upper lip. The vesicles rupture, leaving shallow, painful ulcers that heal over the course of 4 weeks. Several months later, after a skiing trip, similar vesicles develop, with the same pattern of healing. Which of the following is most likely associated with these lesions? a. Biopsy specimen showing squamous epithelial hyperketatosis b. Positive serologic tests for Herpes Simplex 1 c. Peripheral blood smear showing atypical lymphocytes d. Biopsy specimen showing mononuclear inflammatory infiltrate e. Positive serologic tests for Varicella-Zoster virus
Question A 6 year-old boy developed a rash over his chest that began as 0.5-cm, reddish macules. Within 2 days, the macules became vesicles. A few days later, the vesicles ruptured and crusted over. Over the next 2 weeks, crops ov lesions spread to the face and extremities. Which of the following clinical manifestations of this infection is most likely to appear decades later? a. Shingles b. Infertility c. Paralysis d. Congestive heart failure e. Chronic arthritis
Question A 6 year-old boy developed a rash over his chest that began as 0.5-cm, reddish macules. Within 2 days, the macules became vesicles. A few days later, the vesicles ruptured and crusted over. Over the next 2 weeks, crops ov lesions spread to the face and extremities. Which of the following clinical manifestations of this infection is most likely to appear decades later? a. Shingles b. Infertility c. Paralysis d. Congestive heart failure e. Chronic arthritis
Question H. H., a married 15-year-old, white, primigravid adolescent, presented at 31 2/7 weeks' gestation to a community hospital with spotting and preterm labor. Prenatal care was sporadic. At presentation, prior or recent history of herpes was absent. The patient was afebrile. Fetal ascites and possible microencephalywere noted on ultrasound. Bedside fetal heart rate monitor revealed episodes of fetal bradycardia to the 60s during some contractions, with a baseline heart rate in the 150s. The fetal membranes were intact. An emergency Caesarian section was performed. A female infant was delivered. The amniotic fluid was foul-smelling and discolored. The APGAR scores were 0 at 1 and 5 minutes. Resuscitation by an Intensive Care Nursery team was unsuccessful. What is the most likely etiology of the infant’s demise? a. Transplacental transmission of a primary HSV-2 infection b. Transcervical transmission of a primary HSV-2 infection c. Transplacental transmission of a secondary HSV-2 infection d. Transcervical transmission of a secondary HSV-2 infection
Question H. H., a married 15-year-old, white, primigravid adolescent, presented at 31 2/7 weeks' gestation to a community hospital with spotting and preterm labor. Prenatal care was sporadic. At presentation, prior or recent history of herpes was absent. The patient was afebrile. Fetal ascites and possible microencephalywere noted on ultrasound. Bedside fetal heart rate monitor revealed episodes of fetal bradycardia to the 60s during some contractions, with a baseline heart rate in the 150s. The fetal membranes were intact. An emergency Caesarian section was performed. A female infant was delivered. The amniotic fluid was foul-smelling and discolored. The APGAR scores were 0 at 1 and 5 minutes. Resuscitation by an Intensive Care Nursery team was unsuccessful. What is the most likely etiology of the infant’s demise? a. Transplacental transmission of a primary HSV-2 infection b. Transcervical transmission of a primary HSV-2 infection c. Transplacental transmission of a secondary HSV-2 infection d. Transcervical transmission of a secondary HSV-2 infection