Download
1 / 36
360 likes | 385 Views
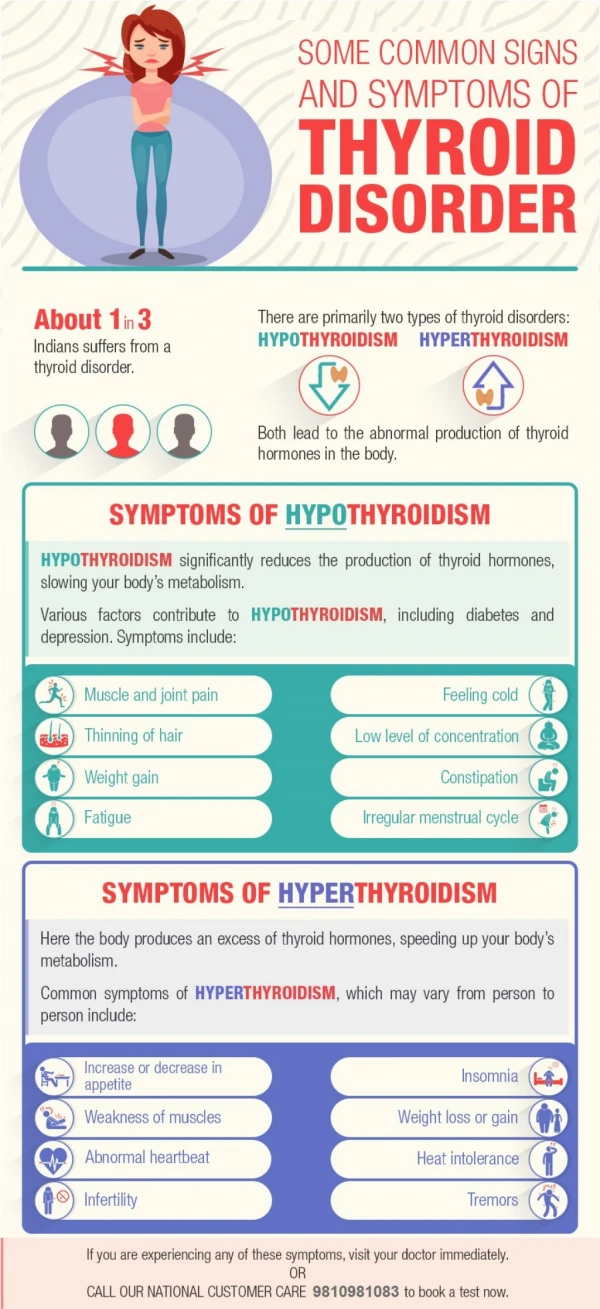
Learn about the thyroid gland, goiter, hypothyroidism, clinical manifestations, and medical management of thyroid disorders.

E N D
Thyroid disorder www..vipinpatidar.wordpress.com
Thyroid Gland • The largest endocrine gland, located in the anterior neck, consists of two lateral lobes connected by a median tissue mass called the isthmus • Thyroid gland is located near the thyroid cartilage of the larynx at the level of C5 to T1. • Butterfly shaped, 25 g weight • The lobes are roughly cone shaped about 5cm long and 3cm wide. • Its highly vascular gland. www..vipinpatidar.wordpress.com
Microscopically it has 2 distinct population of cells: Follicular Cell (produce thyroid hormone) and C cell (produce calcitonin) Thyroid follicles lined with simple cuboidal epithelial (follicular cells) that secretes two hormones, T3 and T4 T4 : 98% and relatively inactive. T3 :cells convert T4 into this form which is much more active. Colloid: incorporates iodine and thryoglobulin to produce thyroid hormone Contd.. www..vipinpatidar.wordpress.com
The Thyroid Gland www..vipinpatidar.wordpress.com
GOITER Enlargement of the thyroid gland may be seen with both hyperthyroidism and hypothyroidism Its generally result of lack of iodine, inflammation, or benign and malignant tumors www..vipinpatidar.wordpress.com
Etiology and risk factors Two major forms of simple goiter are endemic and sporadic. 1. Endemic Goiter- Its cause principally by nutritionally iodine deficiency. It typically occurs in winter months and twice as Prevalent in women as it is in Men. Pregnant women Lactation www..vipinpatidar.wordpress.com
2) Sporadic Goiter Is not restricted to any geographical area Causes include Genetic defect resulting in faulty iodine metabolism Ingestion of large amounts of nutritional goitrogens (goiter producing agents that inhibit thyroxin production) such as Cabbage, soybeans or spinach Medication like Glucocorticoids, Dopamine or lithium www..vipinpatidar.wordpress.com
Clinical manifestations Is confirmed by History and clinical finding and laboratory testes The client may be Euthyroid ( thyroid gland Is functioning normally) as a result of glands attempt to compensate www..vipinpatidar.wordpress.com
Medical Management Iodine and thyroid hormones Endemic Goiter Can be prevented with use of iodized salt. Adults require at least 50 mg of iodine per day www..vipinpatidar.wordpress.com
HYPOTHYRODISM Is a deficiency of TH resulting in slowed body metabolism, Decrease heat production and decreased Oxygen consumption by tissue. Under activity of the thyroid gland may result from Primary thyroid dysfunctions Or it may be secondary to Anterior Pituitary Gland dysfunctions www..vipinpatidar.wordpress.com
Etiology and risk factors • Autoimmune (hashimoto’s thyroditis) • Atrophy of thyroid gland • Therapy of hyperthyroidism • Radioactive Iodine • Thyroidectomy • Medication (lithium, iodine compound) • Radiation www..vipinpatidar.wordpress.com
1. Primary Hypothyroidism TH level are low and TSH level are elevated. This is most common from of primary autoimmune hypothyroidism known as Hashimoto diseases 2. Secondary – Develops when there is insufficient stimulation of normal thyroid gland, Resulting In decrease TSH Level. It may also start as a malfunction of Pituitary or hypothalamus or by Peripheral resistance to TH www..vipinpatidar.wordpress.com
3. Tertiary Or central If the hypothalamus cannot produce thyroid releasing hormone and subsequently does not stimulating the Pituitary to secrete TSH. May be due to the tumor 4. Subclinical hypothyroidism Elevated TSH LEVEL but a normal to low normal level T4 level. www..vipinpatidar.wordpress.com
Clinical Manifestations MILD hypothyroidism May be asymptomatic Lethargy Cold Dry skin Forget fullness, Depression and weight gain www..vipinpatidar.wordpress.com
Sever ( Myxedema) May develop in clients with undiagnosed or undertreated Hypothyroidism that experience stress such as infection, drugs use, Respiratory failure and trauma, Symptoms –dry, waxy type of swelling with abnormal mucin in the skin and other tissue. Non pitting Edema Progressive co2 retention and Coma may develop www..vipinpatidar.wordpress.com
CVS- Decrease HR, Decrease Myocardial o2, Increase peripheral vascular resistance, Hyperlipidemia GI- Decrease peristalsis movement, Anorexia, weight gain, Constipation, Decrease protein metabolism, Increase serum lipids, Delayed glucose uptake Musculoskeletal – Slow movement Integumentary - Dry and scaly skin, Hair that fall out, Thick and brittle nails, Per orbital edema www..vipinpatidar.wordpress.com
Neurologic- Decrease Deep tendon reflexes, Fatigue, Deliberate speech, Apathy, Depression, Short term memory loss. Reproductive - Females: Menorrhagia, Anovulation, Decrease Libido Male: Decrease Libido www..vipinpatidar.wordpress.com
Medical MGTPharmacologic therapy – Levothyroxine is the preferred preparation for treating Hypothyroidism. Dosage based on Serum TSH Concentration Prevention of Medication interaction : TH may interact with other medications. Thyroid hormones may increase blood glucose levels, which may necessitate in the dosage of Insulin or oral Anti diabetic Agent www..vipinpatidar.wordpress.com
Supportive therapy In case sever Hypothyroidism ABG – To determine CO2 Oxygen Saturation Fluid are administered Application of external heat is avoided because increase Oxygen requirements www..vipinpatidar.wordpress.com
NURSING DIAGNOSIS Activity intolerance related to Fatigue Risk for imbalance body temperature Knowledge deficit about the therapeutic regimen for lifelong thyroid replacement therapy www..vipinpatidar.wordpress.com
Hyperthyroidism Refers to over activity of the thyroid gland leading to excessive synthesis of thyroid hormones (graves Disease) It affect women eight time more than men Sometime Its referred as thyrotoxicosis ( Thyroid storm is a potentially fatal acute episode of thyroid over activity characterized by High fever, Sever tachycardia, dehydration and irritability.) www..vipinpatidar.wordpress.com
Diagnosis finding History Physical examination Thyroid gland invariably is enlarged to some Extent Decrease TSH level Increase T3 level www..vipinpatidar.wordpress.com
Medical Management • Anti thyroid hormone • Radioactive iodine • Surgery • Anti thyroid Medication inhibit the synthesis of thyroid hormone • E.G Methimazole, Propothyouracil • Recommended for 18 years age www..vipinpatidar.wordpress.com
Iodine therapy Is prescribed for two reasons To reduce vascularity of the thyroid gland before subtotal and total thyroidectomy and To treat thyroid Strom( Thyrotoxicosis) www..vipinpatidar.wordpress.com
Iodine preparations act temporarily to prevent the release of TH into the circulation by increasing amount TH stored in Gland. I 131 is prescribed mainly for middle age and older client www..vipinpatidar.wordpress.com
Surgical Management Thyroidectomy Removal of thyroid gland may be total or Partial Total- remove thyroid cancer Subtotal –to correct hyperthyroidism and Goiter Indication – Young client Free from any condition like DM, heart disease www..vipinpatidar.wordpress.com
Preparation for subtotal is Extremely Important. If possible the client must be Euthyroid before the operations Administration of antithyroid drugs to suppress secretion of thyroid hormone or iodine preparations to reduce size of gland www..vipinpatidar.wordpress.com
Nursing diagnosis Imbalance nutrition less than body requirements related to Increase metabolic rate Activity intolerance related to Exhaustion Risk for injury(corneal ulceration, Infection and possible blindness related inability to close the eyelid www..vipinpatidar.wordpress.com
THYRODITIS Inflammation of thyroid Gland www..vipinpatidar.wordpress.com
ETIOLOGY Acute Thyroiditis Usually bacterial, Acute thyroiditis can also fungal, Mycobacterial or parasitic. 2. Sub acute thyroiditis May be subacute granulamatous thyroiditis or painless throiditis Usually associated with viral respiratory infection 3. CHRONIC THYROIDITIS(Hashimoto disease) women ( age of 30 to 50 years) www..vipinpatidar.wordpress.com
SIGNS AND SYMPTOMS 1. Acute Anterior Neck Pain and swelling Fever Dysphagia Pharyngeal Pain is often present Treatment Anti microbial agent Fluid replacement Surgical incision and drainage may be needed if an abscess is present www..vipinpatidar.wordpress.com
2. Subacute Painful swelling in the anterior neck that last 1 to 2 months than disappears spontaneously without residual effect. Irritabilility Nervousness Insomnia Weight Loss Fever Chills www..vipinpatidar.wordpress.com
Treatment NSAID drugs used to relive neck Pain B blocking agent may be used to control symptoms of hyperthyroidism Aspirin is avoided if symptoms of hyperthyroidism occurs www..vipinpatidar.wordpress.com
3. Chronic Thyroid Hormone therapy is prescribed to reduce thyroid activity Surgery may be required www..vipinpatidar.wordpress.com