Download
1 / 31
360 likes | 592 Views
Gliomas. OPT. 3-6% of pediatric intracranial tumors 75% in the first decade of life 15-20% of CNS astrocytomas No gender predominance. OPT - Classification. Prechiasmatic Exophitic Diffuse. Prechiasmatic Chiasmatic-hypothalamic. Histopathology. Astrocytic tumors

E N D
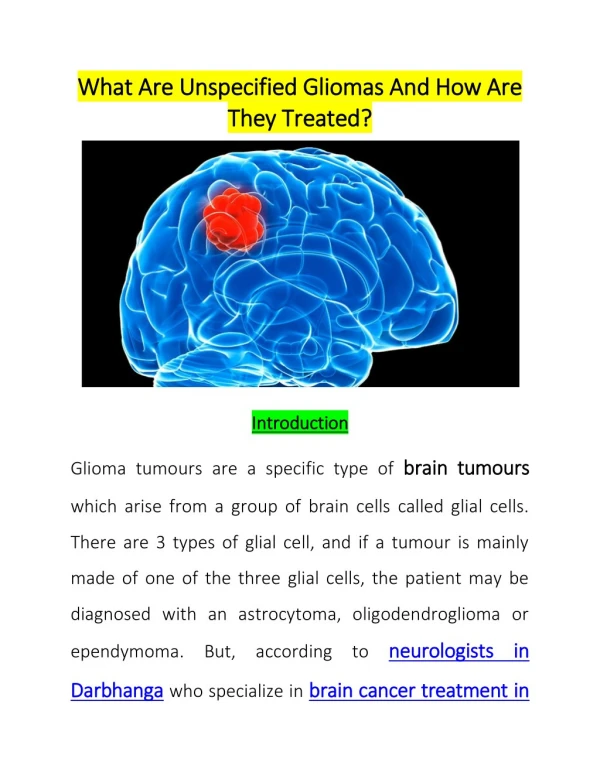
OPT • 3-6% of pediatric intracranial tumors • 75% in the first decade of life • 15-20% of CNS astrocytomas • No gender predominance
OPT - Classification • Prechiasmatic • Exophitic • Diffuse • Prechiasmatic • Chiasmatic-hypothalamic
Histopathology Astrocytic tumors 1.1.1 Astrocytoma - Fibrilary, protoplasmátic, gemystocític 1.1.2 Anaplastic astrocytoma (malignant) GCGB, Gliosarcoma 1.1.3 Multiform gliblastomas 1.1.4 Pilocytic astrocitoma 1.1.5 Pleomorphic xantoastrocitoma 1.1.6 GCSA(Tuberous sclerosis) Pilomixoid astrocytoma (Tihan et al, 1999)
OPT Diagnostic criteria of NF1 National Institutes of Health consensus statement on neurofibromatosis (1987) Six or more café-au-lait macules larger than 5mm in greatest diameter in prepubertal individuals and larger than 15 mm in postpubertal individuals; Two or more neurofibromas of any type or one plexiform neurofibroma; Freckling in the axilary or inguinal region; Optic glioma; Two or more Lisch nodules (iris hamartomas); A distinctive osseous lesion (eg, sphenoid dysplasia or thinning of long bone cortex with or without pseudoarthrosis); A first degree relative (parent, sibling, or offspring) with neurofibromatosis 1 according the above criteria. (Two or more criteria are needed for a diagnosis of NF1) Neurofibromatosis 1 Sporadic
OPT and NF1 Sporadic OPT • Chiasm and hypothalamus • 10 % NF1 • Isolated • Aggressive • IC hypertension OPT and NF1 • Orbital optic nerve • 50-75% of patients have NF1 • Multicentric tumors • Asymptomatic • Indolents • Proptosis / visual deficit
OPT and NF1 “OPG in patients without NF differs significantly from NF-OPG in both imaging features and prognosis. Non NF-OPG and NF-OPG are apparently distinct entities, each warranting a specific diagnostic, clinical and therapeutic approach.” Kornreich L et al., 2001
Optic nerve glioma (ONG) • Proptosis • Painless • Non pulsatile • Visual loss • Optic atrophy/ papilledema • Decreased eye movements
ONG Surgical indications Loss of unilateral vision (blindness) Progressive visual loss Exophtalmos Surgical contraindications Partially preserved vision Moderate proptosis Stable lesions Contralateral extension or chiasmal envolvement
Ch-H tumors : Problems in management • Natural history and course • Number of patients • Variability of treatment options • Lack of prospective of studies • Biologic behavior What is the best treatment ?
Ch-H – Options of treatment • Observation • Stable lesions • NF1 • Surgery • Radical subtotal • Limited • Decompression • Biopsy • Chemotherapy • Radiation therapy
Surgery – Subtotal removal Hoffman, 1983 Albrighth & Selabassi, 1985 Fletcher et al., 1986 Wisoff, 1990
Limited surgery + Chemotherapy After (05/2000) Before (02/1998)
Current trends • Avoid radiation therapy • Delay radiation therapy
Radiation therapy Intelectual impairment Visual impairment Endocrine impairment Moyamoya disease Brain infarction Induced tumors Relapse Older children
Chemotherapy + Radiation therapy 1999 2000 1997 RT 2004 2002
Outcome : Factors affecting long-term survival Increasing age NF1 Chemotherapy Radiation therapy Radiation therapy 69% 10y PFS Grabenbauer et al., 2000 Chemotherapy 34% 5y PFS 89% 5y OS 61% 5y RT FS Laithier et al., 2003
OPT - Conclusions • OPT have an unpredictable course despite histological benignity; • Tumors associated with NF1 have a most favorable outcome; • Age is the most important prognostic factor and younger children have the worst prognosis; • Unilateral ONGs associated with blindness and proptosis are best treated with radical resection; • Subtotal radical surgery of Ch-H tumors is feasible but is associated with a high morbidity; • Chemotherapy seems to be a reasonable alternative as first line treatment of Ch-H tumors; • Prospective, randomized, multicentric studies are needed in order to know the natural history and define the best treatment of OPT.