Download
1 / 1
10 likes | 81 Views
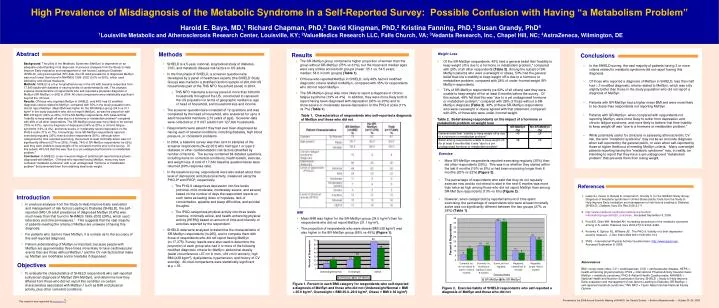
Methods. Results. Abstract. Conclusions. Introduction. 66. 70. 60. 49. 50. 40. Percent of Respondents. 29. 30. Objectives . 21. 21. 20. 13. 10. 0. Underweight/Normal. Overweight. Obese. Exercise Habits. SR-MetSyn. No SR-MetSyn. This research was supported by.

E N D
Methods Results Abstract Conclusions Introduction 66 70 60 49 50 40 Percent of Respondents 29 30 Objectives 21 21 20 13 10 0 Underweight/Normal Overweight Obese Exercise Habits SR-MetSyn No SR-MetSyn This research was supported by High Prevalence of Misdiagnosis of the Metabolic Syndrome in a Self-Reported Survey: Possible Confusion with Having “a Metabolism Problem” Harold E. Bays, MD,1 Richard Chapman, PhD,2 David Klingman, PhD,2 Kristina Fanning, PhD,3 Susan Grandy, PhD4 1Louisville Metabolic and Atherosclerosis Research Center, Louisville, KY; 2ValueMedics Research LLC, Falls Church, VA; 3Vedanta Research, Inc., Chapel Hill, NC; 4AstraZeneca, Wilmington, DE • The SR-MetSyn group contained a higher proportion of women than the group without SR-MetSyn (75% vs 61%), but the mean and median ages were very similar across both groups (mean: 55.1 vs. 54.5 years; median: 54.0 in both groups) (Table 1). • Of those who reported MetSyn in SHIELD, only 48% had ≥3 modified diagnostic criteria related to MetSyn, compared with 35% for respondents who did not report MetSyn. • The SR-MetSyn group was more likely to report a diagnosis of chronic fatigue syndrome (19% vs 4%). In addition, they were more likely both to report having been diagnosed with depression (36% vs 20%) and to show severe or moderately severe depression on the PHQ-9 scale (11% vs 7%) (Table 1). Background: The utility of the Metabolic Syndrome (MetSyn) is dependent on an adequate understanding of its diagnosis. In previous analyses from the Study to Help Improve Early evaluation and management of risk factors Leading to Diabetes (SHIELD), using self-reported (SR) data, the US adult prevalence of diagnosed MetSyn was much lower than found in NHANES 19992002 (0.6% vs 26%), which used laboratory and clinical measures. Methods: SHIELD is a 5-yr longitudinal survey in the US with baseline responses from 17,640 adults with diabetes or varying levels of cardiometabolic risk. This analysis explores characteristics of respondents who self-reported a physician diagnosis of MetSyn (SR-MetSyn; n=265) in 2004. All cited comparisons were statistically significant beyond the .05 level. Results: Of those who reported MetSyn in SHIELD, only 48% had ≥3 modified diagnostic criteria related to MetSyn, compared with 35% in the study population who did not report MetSyn. Mean BMI was higher for the SR-MetSyn group (34.0 vs 31.1 kg/m2 in the study population who did not report MetSyn), as was the proportion with BMI ≥30 kg/m2 (64% vs 49%). Of the SR-MetSyn respondents, 49% believed that “inability to keep weight off was due to a hormone or metabolism problem" compared with 28% of all other respondents. The SR-MetSyn group was more likely to be women (75% vs 61%), report a diagnosis of depression (36% vs 20%) or chronic fatigue syndrome (19% vs 4%), and show severe or moderately severe depression on the PHQ-9 scale (11% vs 7%). Interestingly, more SR-MetSyn respondents reported exercising regularly (35%) than did other respondents (30%), although when categorized by time reported exercising, the percent at least minimally active was not significantly different (27% vs 28%). Finally, 74% of SR-MetSyn respondents (vs 62%) said they were unable to keep weight off for at least 6 months prior to the survey. Of this subset, 40% felt that this was “due to a yet undiagnosed hormone or metabolism problem." Conclusion: In SHIELD, a very low percentage of patients self-reported having been diagnosed with MetSyn. Of those who reported having MetSyn, many may have confused “metabolic syndrome” with a yet undiagnosed “hormone or metabolism problem” that prevented them from attaining ideal body weight. • SHIELD is a 5-year, national, longitudinal study of diabetes, CVD, and metabolic disease risk factors in US adults. • In the first phase of SHIELD, a screener questionnaire developed by a panel of healthcare experts (the SHIELD Study Group) was mailed to a stratified random sample of 200,000 US households (part of the TNS NFO household panel) in 2004. • TNS NFO maintains a survey panel of more than 600,000 households throughout the US, constructed to represent the US population in terms of geographic residence, age of head of household, and household size and income. • The screener questionnaire consisted of 12 questions and was completed by the head of household, who answered for up to 4 adult household members (18 years of age). Screener data were collected on 211,097 adults from 127,420 households. • Respondents were asked if they had ever been diagnosed as having each of several conditions, including diabetes, high blood pressure, or cholesterol problems. • In 2004, a baseline survey was then sent to samples of the screener respondents (N=22,001) who had type 1 or type 2 diabetes or other cardiometabolic risk factors (stratified by number of factors). The survey contained 64 detailed questions, including items on comorbid conditions, health beliefs, exercise, and weight loss. A total of 17,640 baseline questionnaires were returned (80% response rate). • In the baseline survey, respondents were also asked about their level of depression and physical activity, measured using the PHQ-94 and IPAQ5, respectively. • The PHQ-9 categorizes depression into five levels (minimal, mild, moderate, moderately severe, and severe) based on the number of days the respondent reports on such items as feeling down or hopeless, lack of concentration, appetite and sleep difficulties, and suicidal thoughts. • The IPAQ categorizes physical activity into three levels (inactive, minimally active, and health-enhancing physical activity [HEPA]) based on amount of time and intensity of activities reported by the respondent. • SHIELD data were analyzed to determine the characteristics of SR-MetSyn respondents (n=265), and to compare them with those of respondents who did not report having MetSyn (n=17,375). Survey results were also used to determine the proportion of each group who had 3 or more of the following modified diagnostic criteria for MetSyn: abdominal obesity (waist circumference >97 cm in men, >89 cm in women), high BMI (≥28 kg/m2), dyslipidemia, hypertension, and history of CV event(s). All cited comparisons were statistically significant at p <.05. Table 1. Characteristics of respondents who self-reported a diagnosis of MetSyn and those who did not References • In previous analyses from the Study to Help Improve Early evaluation and management of risk factors Leading to Diabetes (SHIELD), the self-reported (SR) US adult prevalence of diagnosed MetSyn (0.6%) was much lower than that found in NHANES 19992002 (26%), which used laboratory and clinical measures.1 This suggests that the vast majority of patients meeting the criteria of MetSyn are unaware of having this diagnosis. • For patients who claim to have MetSyn, it is unclear as to the accuracy of this self-reported diagnosis. • Patient understanding of MetSyn is important, because people with MetSyn are approximately three times more likely to have cardiovascular events than are those without MetSyn,2 and the CV risk factors that make up MetSyn are modifiable and/or treatable if diagnosed. BMI • Mean BMI was higher for the SR-MetSyn group (34.0 kg/m2) than for respondents who did not report MetSyn (31.1 kg/m2). • The proportion of respondents who were obese (BMI ≥30 kg/m2) was also higher in the SR-MetSyn group (66% vs 49%) (Figure 1). • To evaluate the characteristics of SHIELD respondents who self-reported a physician diagnosis of MetSyn (SR-MetSyn), and determine how they differed from those who did not report this condition on certain characteristics associated with MetSyn,3 such as BMI and physical activity, plus other comorbid conditions. Figure 1. Percent in each BMI category for respondents who self-reporteda diagnosis of MetSyn and those who did not (Underweight/Normal = BMI< 25.0 kg/m2, Overweight = BMI 25.0–29.9 kg/m2, Obese = BMI ≥ 30 kg/m2) Presented at the 2006 Annual Scientific Meeting of NAASO, the Obesity Society • Boston, Massachusetts • October 20–24, 2006



















