Download
1 / 19
210 likes | 545 Views
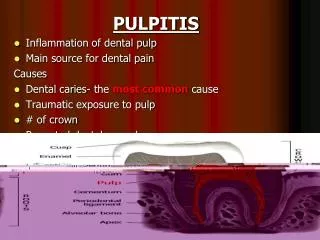
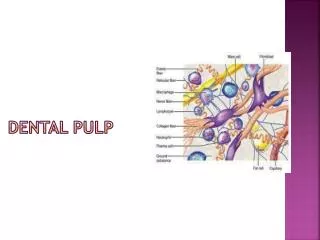
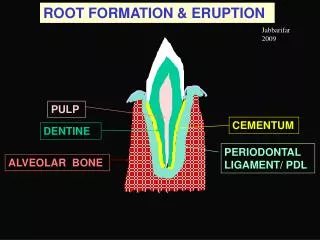
Disorder of the dental pulp Pulpitis. Pulp tissue is composed of delicate C.T. , blood vessels , lymphatics , myelinated & unmyelinated nerve fibers , & undifferentiated cells. Pulpitis : inflammation of the dental pulp tissue .

E N D
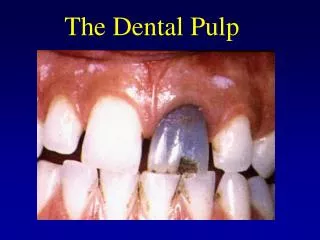
Disorder of the dental pulp Pulpitis
Pulp tissue is composed of delicate C.T. , blood vessels , lymphatics , myelinated & unmyelinated nerve fibers , & undifferentiated cells. Pulpitis : inflammation of the dental pulp tissue . inflammatory process in the pulp is basically the same as elsewhere in the body but the process may be modified by various factors.
The causes of pulpitis 1.Microbial Bacteria generally reach the pulp as a result of dental caries. Inflammation of the pulp starts before organisms in the carious dentine reach the pulp. showing that the initial pulp reactions follow the diffusion of soluble irritants through the dentine .
2.Chemical Irritant substances may be directly applied to an exposed pulp. or may diffuse through the dentine after the insertion of a restorative material . 3.Thermal Frictional heat evolved during cavity preparation is a significant pulp irritant . Large metallic restoration .
4.Barotrauma (aerodontalgia) pain has been described by air crew flying at high altitudes and in divers subjected to too rapid decompression following deep sea diving .This pain has been attributed to the formation of nitrogen bubbles in pulp tissues or vessels.
Classification of pulpitis : • clinical basis into a number of different types. such as acute or chronic, open or closed. or • 2.pathological basis , partial or total, exudative or suppurative. These divisions are somewhat artificial and confusing since inflammation of the pulp presents a continuous spectrum of change .
Clinical features Presents clinically as pain which the patient may have difficulty in localizing to a particular tooth. the pain often radiating to the adjacent jaw and on some occasions into the face, the ear. or the neck. The pain may be continuous for several days or may occur intermittently over a longer period.
Focal reversible pulpitis ( pulpal hyperemia ) : Clinically: the patient complain from pain & sensation during thermal changes – especially cold- the pain & sensation immediately disappear after removal of irritant . The teeth affected are having either deep cavity or metallic filling with inadequate isolation. Histologically : dilated blood vessels with slight odema & exudates. Treatment : removal of irritant before extensive pulpitis progress
Acute pulpitis : A severe throbbing pain, at times lancinating in type, precipitated by hot or cold stimuli or a recumbent position, and commonly keeping the patient awake. The pain generally lasts for about 10-15 minutes .
Histologically : increase dilation of B.V. , migration of inflammatory cells within the pulp tissue & if the inflammation persist , focal pulp abscess can be seen due to progressive accumulation of neutrophil leucocytes. Treatment : 1.root canal treatment 2. extraction if the tooth is hopeless 3.in children we start with pulptomy.
Chronic pulpitis : Spontaneous attacks of dull aching pain, lasting for an hour or two. the affected tooth shows reduction to thermal changes. Histologically : there are various types of chronic inflammatory cells , mainly lymphocyte & plasma cells . also prominent capillaries & fibroblastic activity which lead to encircle area of inflammation.
Investigations have shown that there is little or no correlation between the clinical features and the type or extent of pulp inflammation as shown by histological examination. An absence of symptoms is not evidence of a normal pulp as pulp death following pulpitis may occur with no previous history of pain.
Clinically is weather pulpitis is reversible or irreversible. as this will determine the management of the affected tooth. This decision is based on factors such as the age of the patient, the size of the carious lesion, the presence or absence of symptoms, pulp vitality tests, radiographic evidence, and direct observation during operative procedures.
Pulp polyp wide-open carious cavities and a good apical blood supply, pulpitis may be associated with a hyperplastic granulation tissue response. The granulation tissue grows out of the boundary of the pulp chamber to form a pulp polyp and described as chronic hyperplastic pulpitis . The polyp may become epithelialized by oral epithelial cells present in the saliva .
Clinically: At first an ulcerated pulp polyp presents dark red, yellow-flecked fleshy mass protruding from the pulp chamber. which bleeds readily on probing then epithelialized polyp become firmer, pinkish-white in color, and does not bleed readily, and usually devoid of sensation on gentle probing.
Pulp necrosis May follow either pulpitis or a traumatic injury to the apical blood vessels cutting off the blood supply to the pulp. 1. coagulative type of necrosis is seen after ischaemia. but if the necrosis follows pulpitis then breakdown of inflammatory cells may lead to 2. liquefactive type of necrosis which may become infected by bacteria from caries.
Gangrenous necrosis of the pulp is usually associated with a foul odour when such infected pulps are opened for endodontic treatment. Pulp necrosis has also been described in patients with sickle cell anemia following blockage of the pulp microcirculation by sickled erythrocytes